 On March 13th the Food and Drug Administration finally approved the WATCHMAN device for prevention of stroke in patients with atrial fibrillation (AF) in the USA. The WATCHMAN is a percutaneous implantable device designed to occlude the left atrial appendage (LAA). It's been a long journey for this device, now owned by Boston Scientific and six years have passed since the publication of the first clinical trial, PROTECT-AF.
In AF 90% of cardiac thrombi are thought to originate in the LAA. A strategy to occlude or remove the LAA is an attractive target to reduce stroke risk and avoid the need for lifelong anticoagulation. Already some cardiac surgeons routinely remove the LAA at the time of cardiac surgery. There is a clinical trial, which will report in 2016, testing the hypothesis that this additional surgical procedure will reduce the risk of stroke. Even if this trial is positive however it will only be relevant to patients undergoing cardiac surgery for other reasons and not open to the vast majority of patients with AF. The PROTECT-AF trial showed the device was non-inferior to warfarin for stroke prevention but there was a high rate of serious procedure related complications. Interestingly when the data was analysed looking at earlier versus later implants the complication rates decreased markedly as operator experience increased. This was confirmed in a later follow-up registry study and further date came from another clinical trial called PREVAIL. If you want to read all of the clinical trial data in detail then the summary on the FDA website is excellent. The clinical trials with the LAA device are very small in comparison to modern pharmaceutical trials. For the NOACs in AF we have four mega-trials and a meta-analysis with 102,000 patients worth of date. Compare this to the PROTECT-AF trial with its mere 707 patients. It is therefore not surprising that the confidence intervals in this device trial are very wide. Interestingly the major benefit in the PROTECT-AF trial was the reduction in the risk of intracranial bleeding. Since this safety endpoint is significantly reduced in patients taking NOACs it would be more appropriate to be considering comparing the LAA occlusion devices with NOACs rather than Warfarin. Now the device has been approved by the FDA we will see a surge in the rate of implants in USA. In Europe already the implant rate is very high in Germany a phenomenon very commonly seen in this country when it comes to the treatment of patients with devices and interventional procedures in cardiology. In the UK some centres such as the Royal Brompton Hospital have implanted over 100 devices. Interestingly NHS England's specialist commissioning have recently selected two different tertiary centre units to perform this procedure in London. Perhaps they didn't consider that the association with operator experience and procedural complication rates was important. Personally I think that the LAA occlusion device will end up as a niche procedure which has a role for those patients with a high CHADSVASC score who are unable to take oral anticoagulants. It is vital going forward that more research takes place with the WATCHMAN and other LAA occlusion devices to determined whether their potential promise will be delivered. At this point we are right to ask Quis custodiet ipsos custodies?
0 Comments
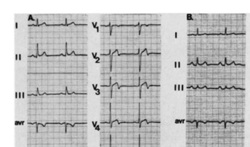 In people admitted to the hospital with cardiac chest pain a subgroup is recognized on the basis of a characteristic ECG change that predicts a high risk of impending extensive anterior myocardial infarction. The ECG has a highly characteristic ST-T segment change in the chest leads and at angiography patients usually have a critical stenosis in the proximal left anterior descending coronary artery.
In the original paper published in 1982 in the American Journal of Cardiology they found 26 patients out of 145 consecutive admission had this typical pattern. The description was of abnormal ST-T segments in leads V2 and V3 consisting of an isoelectric or minimally elevated (1 mm) take-off of the ST segment from the QRS complex, a concave or straight ST segment passing into a negative T wave at an angle of 60 to 90 degrees, and a symmetrically inverted T wave. Twenty-five of the 26 patients also had a typical pattern in lead V1: an isoelectric or minimally elevated (1 mm) take-off of the ST segment and a concave or straight ST segment passing into the first part of the T wave at an angle of approximately 135 degrees, followed by T wave inversion. In addition, 22 had an ST-T segment pattern in lead Vl, and sometimes V2 and V3, consisting of a take-off of the ST segment from the QRS complex below the isoelectric line and a convex ST segment passing into a negative T wave at an angle of about 120 degrees with a deep symmetrically inverted T wave. As with many things a picture says a thousand words and the figure illustrated above shows the two patterns. The original paper published in 1982 shows the natural history of this condition if managed conservatively with beta blockers and GTN. They had 145 patients consecutively admitted with chest pain of which 18% had the characteristic ECG pattern and 75% of them who were not operated on developed an extensive anterior wall infarction within a few weeks after admission. The authors recommended that patients with this ECG pattern should have urgent coronary angiography and revascularization. Cardiologists now refer to this ECG pattern as a Wellens ECG or Wellens syndrome. In a patient with symptoms of chest pain it should prompt the patient to be admitted to hospital irrespective of the troponin level and urgent coronary angiography arranged. This is certainly a situation where coronary revascularisation will reduce the risk of myocardial infarction.  Do you remember the children's song "I know an old lady who swallowed a fly?" She swallowed a spider to catch the fly, then a bird to catch the spider, she swallowed a cat to catch the bird etc. Eventually she swallowed a horse - and as the song goes "She dead of course!"
This song reminded me of a recent patient. A middle aged man with no medical problems, normal blood pressure and a cholesterol of 5.4. He happened to have the "good fortune" of being sent for a routine executive medical. The ECG was abnormal showing left axis deviation and a Q wave in lead V2. The ECG report suggested cardiology referral and recommended an echocardiogram. The echocardiogram showed possible septal hypokinesia with good LV function and normal valves. The echo led to a CT coronary angiogram which showed a normal left coronary and a 50% stenosis in the mid right coronary artery. The CT led to an exercise ECG which showed 1mm ST depression infero-laterally at 6 minutes of exercise. The exercise ECG led to an invasive angiogram which showed a moderate mid right coronary stenosis. The angiogram led to FFR measurement of the lesion with a FFR at maximum hyperaemia of 0.74. The FFR led to a coronary stent being implanted and the prescription of dual antiplatelet therapy, ACE inhibitors, intensive statins and beta blockers. The patient was asymptomatic physically but anxious. How would he know if coronary disease were to occur in the future, when should he arrange another angiogram? It seems that one thing leads to another. One test leads to the next and then the next and so on. The patient had evidence of coronary disease and it was demonstrated to be flow limiting so according to the best evidence from the studies it is possible to justify all the steps that were taken. Has all of this testing resulted in an improvement in the patient's health, is the risk of death, myocardial infarction or need for urgent revascularisation reduced. Will there be unwanted effects of the drugs being used. Did the patient really benefit from stent insertion especially as he had never had any symptoms of chest pain? When people have health screening it is very important that they understand what the possible outcomes of doing these investigations. |

Dr Richard BogleThe opinions expressed in this blog are strictly those of the author and should not be construed as the opinion or policy of my employers nor recommendations for your care or anyone else's. Always seek professional guidance instead. Archives
August 2023
Categories
All

|
 RSS Feed
RSS Feed