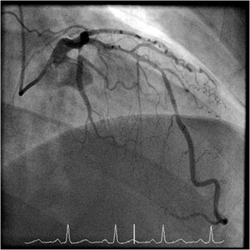
 When a patient has a coronary angiogram the cardiologist will report the results in terms of the degree of narrowing of the arteries. For example a 60% stenosis in the LAD, a 40% stenosis in the circumflex. But what does that really mean? Is the stenosis flow limiting? Is it responsible for the patients symptoms? Is the lesion prognostically significant? Should a stent be place? Is a bypass indicated? Many questions but the fundamental one is: "Would this patient's outcome be better with or without revascularisation or is medical therapy more appropriate?" When there is mild or critical coronary artery disease then the decision making is straightforward. However in many cases there are moderate areas of coronary narrowing. Showing the angiogram to several cardiologists will usually result in differing opinions about whether a lesion is flow limiting or not. For some cardiologists the "Oculostenotic reflex" is already potentiated leading to "iatrogenosis fulminans." In 1995 Steve Nissen and Eric Topol wrote about cardiologists preoccupation with luminography and eloquently showed how lesion assessment with angiography performed very poorly compared to intravascular ultrasound. They also wrote of the dissociation between the angiogram and clinical outcome and called for a shift in our with luminology towards measures that improve survival, freedom from myocardial infarction and symptoms of angina. Whether a coronary lesion is flow limiting is not just dependent on the degree of arterial stenosis but also on the amount of cardiac muscle supplied, the presence of collateral vessels, the length of the lesion and the function of the endothelium. Some of these factors can be assessed subjectively by angiography but others cannot. What is required is a more functional or physiological assessment. Cardiologists have fooled themselves for too long that they are able to determine the functional significance of a moderate coronary stenosis from the angiogram alone. Recent data using the pressure wire has challenged some of this thinking although there are still some sceptics. The FAME studies showed that use of the pressure wire to measure fractional flow reserve (FFR) could be useful to help in selecting the appropriate therapy and guiding coronary revascularization in patients referred for a percutaneous coronary intervention (PCI) procedure. Very recently a real world study has been published using FFR in patients referred for diagnostic angiography and looking at its impact on the decisions involved in revascularization. In this study patients referred for diagnostic angiography had a treatment plan for intermediate lesions (35-65% by eye) made on the basis of the angiography alone. 55% of patients were recommended to receive medical therapy and 45% revascularization (PCI, 38%; CABG, 7%). FFR measurement was then performed with the pressure wire and after this 58% of patients were recommended for medical therapy and 42% for revascularization (PCI, 32%; CABG, 10%). The results were not so different overall but in individual patients the FFR strategy changed the recommended treatment in 43% of cases. Reclassification was observed in 33% medical patients, 56% of PCI patients and 51% of CABG patients. These results are hugely important since they indicate that even experienced cardiologists are unable to judge the flow limiting nature of moderate lesions. In the initial medical treatment group one third of patients met FFR criteria for revascularisation. In the PCI group, half of patients were due to receive inappropriate or a less optimal type of revascularisation. In the surgical group over half of patients could have avoided an operation. What this study is telling us is that using the eyeball technique to judge the severity of coronary disease is not the best way to decide on a management plan for cardiac patients. If the practice of using a pressure wire became standard in diagnostic coronary angiograms it would lead to more patients receiving medical therapy, less receiving angioplasty and more patients having CABG. The effects on the economics of management of coronary disease are complex. Assuming everyone gets medical therapy then the cost of the increased CABG although a more expensive procedure is offset by the reduction in expenditure on angioplasty. The repeat revascularisation costs are likely to be lower since this has been shown routinely in most of the CABG versus PCI studies. There is of course the cost of the pressure wire for every case. Overall the most improtant thing is that the patient receives the most appropriate treatment and not at the mercy of the oculostenotic reflex. 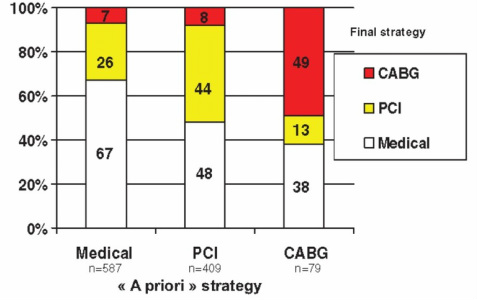
1 Comment
 In 2010 NICE published a guideline on Chest Pain of Recent Onset. This was an important document for GPs and cardiologists. It has been widely cited and has had an effect on how Rapid Access Chest Pain clinics operate. NICE used their usual cost-effectiveness approach to review and then recommend which cardiac investigations were most appropriate in the assessment of patients with chest pain. Some of the recommendations e.g. to not use exercise treadmill testing to assess patients have been largely ignored by many cardiologists but the guidelines have stimulated an increase in the use of non-invasive imaging tests such as CT coronary angiography, myocardial perfusion scanning and stress echocardiography. A recent article in the BMJ “Rational Imaging” series sought to review the investigation of stable chest pain of suspected cardiac origin. Essentially this was a rehash of the 2010 NICE guidelines with focus on the estimation of likelihood of a patient having coronary artery disease and a strong bias to recommended CT and cardiovascular MR imaging (not surprising since all of the authors have specialist interests in this discipline). I think it is time to redress the balance around imaging investigations and critically review the NICE guideline approach. The BMJ article describes the following case: A 45 year old man, who was a non-smoker and did not have diabetes or hyperlipidaemia, presented to his doctor with chest discomfort after exercise. There were no relevant findings on clinical examination and resting electrocardiography (ECG) results were normal. On the basis of age, sex, risk factors, and symptoms, the patient’s pre-test probability of coronary artery disease was 21% and he was referred for calcium scoring. The calcium score was 11 and he proceeded to computed tomography coronary angiography, which identified a 70% stenosis of the left anterior descending coronary artery. Adenosine stress perfusion cardiac magnetic resonance imaging showed reduced perfusion of the septum within the territory of the left anterior descending coronary artery. He was managed for stable angina on the basis of these findings. I see very many patients with this type of clinical presentation and my approach would not be that recommended by the authors of this article. My clinical impression is that the patient has angina. I would recommend treatment with 75mg aspirin, a beta blocker and to give a GTN spray. I would recommend that the patient has an invasive coronary angiogram. The angiogram is done to define the pattern of coronary artery disease and to decide on the correct approach to further management which may or may not involve revascularisation. The patient starts treatment as soon as the diagnosis of angina is made to improve symptoms and reduce risk of cardiovascular events. So the diagnosis and treatment plan for the patient is completed in a timely manner and with a single test rather than three different tests. NICE and this rational imaging review recommend a different approach. First you estimate the likelihood of coronary artery disease. How? The authors use the table in the NICE guidelines (see below) and say it’s 21%. On that basis they recommend a CT calcium score. I would take issue with this on two counts. First I think the patient’s symptoms are consistent with angina and therefore his predicted risk, according to the NICE guidelines, is much higher at 51%. Second there is evidence that in a younger patient coronary artery disease may occur in the absence of calcification of the coronary arteries. So a zero calcium score does not confidently exclude coronary artery disease in a symptomatic patient. Calcium scoring of the coronary arteries is a relatively quick, cheap and simple test which is entirely non-invasive. CT coronary angiography involves pre-treatment of the patient usually with beta blockers to reduce the heart rate to 60 and pre-assessment of the renal function as intravenous contrast will be administered. The patient then has a CT coronary angiogram and now we see that rather than the predicted 21% chance of having coronary disease the patient does actually have the disease. He then has an adenosine perfusion cardiac magnetic resonance scan (not very widely available, certainly expensive but as all of the authors are experts in CMR scanning not surprising). This demonstrates cardiac ischaemia which is not surprising since there is a flow limiting lesion in a coronary artery and the patient has symptoms of chest pain. After that the patient is managed for stable angina. This management, not discussed in the article, most likely involves an invasive angiogram and consideration of angioplasty to relieve symptoms if not controlled by medical therapy. Whilst the approach described by the authors might be appropriate for an asymptomatic patient it seems a long and complicated route to identify and treat the disease which most cardiologists could have predicted was there from simply taking a proper history. The best predictor of the presence of obstructive coronary artery disease is the presence of symptoms of angina. That’s not to say that patients without angina don’t have coronary artery disease. They do and many patients with significant coronary artery disease do not have classical symptoms of angina. In my view there are two principle questions to address. First, what is the cause of the patient’s symptoms of chest pain? If the answer is coronary artery disease then appropriate investigation needs to be undertaken. If the answer to this is no, then apart from trying to determine the non-cardiac cause of chest pain the other question is could this patient have underlying coronary artery disease? If the risk is high then appropriate preventative measures need to be recommended with regards to lifestyle and other risk factors. It is frustrating that many patients leave a chest pain clinic or accident and emergency department with a diagnosis of “non-cardiac chest pain." 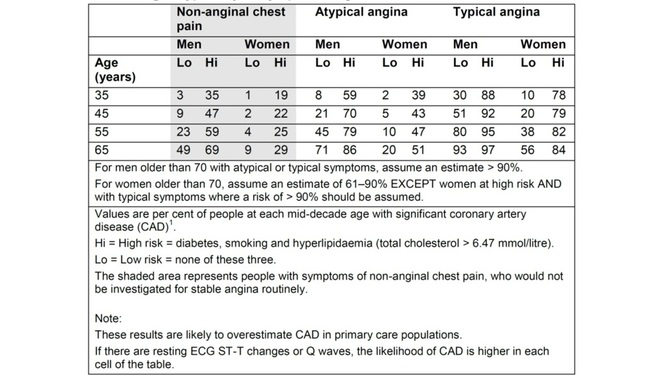 Table from NICE Chest Pain Guidelines. Note the limited ages available for lookup and that "High Risk is defined as diabetes AND smoking AND hyperlipidaemia. This is often misquoted as it has been in the BMJ Rational Imaging Article as diabetes OR smoking OR hyperlipidaemia. Using the table in the NICE guidelines to predict risk of coronary artery disease is risky business itself. First only mid-decade ages are given so most patients fall between the categories of risk. Then with the risk factors you either have none and are low risk or you are a diabetic smoker with a cholesterol of >6.47mmol/l (it’s a strange number because the original study is from the USA and used an LDL cut off of >250mg/dl) and you are high risk. A single risk factor doesn’t count as high risk and so it is impossible from the table to estimate the risk for the majority of patients we see.
You can get around this by going back to the original paper which contains the risk model equations and building your own model to allow the exact age and individual risk factors. NICE didn’t do this in the guideline because it would be too complicated but it is ideally suited to an online version which I will publish soon on my website. Sadly however that doesn’t solve the problem. If you deconstruct the data in the table and go back to the original source you will be surprised and also disappointed. The original data comes from a paper published in the Annals of Internal Medicine in 1993 and reports the experiences of the Duke University Chest Pain Clinic. At Duke they collected sequential data on 1030 patients attending the clinic who were assessed for suspected ischaemic heart disease. 168 patients went on to have a coronary angiogram and from this cohort the risk prediction model was built and this produced the data in the table above. The tiny small sample size and the population on which it is based should make anyone use the NICE table with great caution. One wonders how many 35 year old females with no risk factors and typical angina were really studied by angiography in the 1980's when the data was collected. Certainly to use the numbers as a basis for determining the behaviour of different non-invasive investigation techniques would lead to a very high likelihood of inaccuracy. In the end there is as they say no substitute for experience. The most appropriate way to manage a patient with chest pain is for the assessment to be performed by an experienced cardiologist who can recommend the most appropriate strategy for that individual patient to get to the diagnosis and formulate a treatment plan as quickly and efficiently as possible. References: National Institute for Health and Care Excellence. Chest pain of recent onset: assessment and diagnosis of recent onset chest pain or discomfort of suspected cardiac origin. CG95. 2010. Declan P O’Regan, Stephen P Harden, Stuart A Cook, Investigating stable chest pain of suspected cardiac origin BMJ 2013;347:f3940 Pryor DB, Shaw L, McCants CB et al. (1993) Value of the history and physical in identifying patients at increased risk for coronary artery disease. Annals of Internal Medicine 118(2):81–90.  This week saw the publication of another large clinical trial investigating the effects of dietary supplementation with omega-3 containing fish oil to prevent cardiovascular disease. The use of fish oil to promote good health goes back many hundreds of years however interest grew in the 1960's when there were reports of very low levels of coronary heart disease in Greenland Eskimos. This was attributed to a diet that was rich in marine omega–3 fats and led to the hypothesis that omega-3 supplementation would prevent cardiovascular disease. Today omega-3 is synonymous with good health and supplements are taken widely in the belief that they will prevent heart disease. There has been a large amount of clinical research but much controversy remains as to the effectiveness of these supplements. So what is the evidence that supplementing the diet with fish oils prevents heart disease and are we overlooking other important aspects of the Eskimo diet which might be responsible for their good health? Does fish oil prevent high risk people getting heart disease? A recent study published in NEJM randomised 12,513 patients to take either omega-3 supplements or placebo. The trial subjects had multiple cardiovascular risk factors or clinical evidence of vascular disease. After 5 years 11% of subjects had experienced cardiovascular events but there was no effect of omega-3 treatment. Does fish oil prevent recurrent heart disease after heart attack? In the GISSI-P study diet was supplemented with omega-3 rich fish oil in people who had recently had a heart attack. Over 3.5 years there was a difference of just 1.3% in favour of fish oil in the combined end point of death, non-fatal MI and non-fatal stroke. This study was conducted about 20 years ago and the treatment of patients post MI is now very different. Only 40% of patients were on beta-blockers or ACE inhibitors and only a 25% underwent stenting or had coronary bypass surgery. Clopidogrel, now almost always used after an MI, was not available at that time and the statin mega trials had not been published so at the start of the trial only a few patients were treated with these drugs. The overall effect of omega-3 supplementation was small and of low clinical significance. This was further confirmed in a the more contemporary Alpha-Omega Study published in 2010 which again showed no benefit with omega-3 fatty acid rich margarines. A Cochrane systematic review of trials included 36,913 participants and 41 cohort analyses. Pooled trial results did not show a reduction in the risk of total mortality or combined cardiovascular events in those taking additional omega-3 fats no significant effect of omega-3 fats. Although omega-3 supplementation was originally recommended by NICE most local cardiac networks and guidelines groups have strongly indicated that omega-3 is not a high priority to be prescribed for patients  Why doesn't omega-3 prevent heart disease?
Whilst there is biochemical and observational research to suggest that omega-3 fatty acids are beneficial to prevent cardiovascular disease the large controlled clinical trials have been very disappointing. The original fish oil hypothesis was formed following the observation of a very low level of cardiovascular disease in Inuit Eskimos. The diet of an Eskimo would be regarded, at first glance, as extremely unhealthy. It contains a large amount of animal protein and fat. The amount of carbohydrate and sugar is very low. The Eskimo diet is like that of a carnivorous animal and very rich in omega-3 fatty acid. Most researchers have focused on the high omega-3 content of the diet forgetting the high fat and protein content. Because of the link between cholesterol and fat to coronary artery disease, the lack of carbohydrate and sugar in the diet were quietly forgotten. So to pick on one component, albeit present at high level in the diet, and expect that supplementing it into a completely different high carbohydrate Western diet would lower heart disease is not particularly credible. Recently the book by Dr John Yudkin - "Pure, White and Deadly has been republished. The thesis of this book was that the rise in coronary heart disease is due to the increased consumption of sugar in the Western diet rather than the traditional belief that it is related to the consumption of saturate fat. It is interesting that the Eskimo diet was very rich in fat and meat but low in sugar. Perhaps if we want to obtain the same low risk of heart disease of the Eskimos we need to follow their marine diet more closely. References: n–3 Fatty Acids in Patients with Multiple Cardiovascular Risk Factors: The Risk and Prevention Study Collaborative Group N Engl J Med 2013; 368:1800-1808 May 9, 2013 DOI:10.1056/NEJMoa1205409 n–3 Fatty Acids and Cardiovascular Events after Myocardial Infarction Daan Kromhout, M.P.H., Ph.D., Erik J. Giltay, M.D., Ph.D., and Johanna M. Geleijnse, Ph.D. for the Alpha Omega Trial Group N Engl J Med 2010; 363:2015-2026 November 18, 2010 DOI: 10.1056/NEJMoa1003603 The study of ancient medical history usually relies on documents and objects as sources. Ancient Egyptian medicine is unique because in addition to the ten medical papyri which date from 1550 BCE and objects and tomb drawings historians and biologists have had unparalleled access to human preserved material in the form of mummified remains. 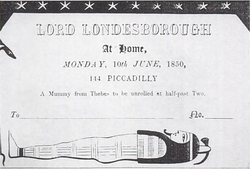 In the 19th century it was not uncommon for people to be invited to the "unrolling" of a mummy brought back from excavations in the middle east. More recently multi-disciplinary teams have come together to investigated mummies in museum collections and from newly excavated sites using non-invasive and tissue sparing techniques such as CT scanning, endoscopy and molecular biology. This has allowed the study of wrapped mummies and allowed these remains to be preserved intact. This work has led to some fascinating insights into the types of diseases present in our ancient ancestors who live over 4000 years ago. For the cardiologist coronary artery disease and atheroscleorsis are often thought of as 20th century problems caused by diet, smoking habits, exercise patterns and lifestyle. It is often said that if we were able to get back to a more primitive diet and to have the daily exercise of the ancient hunter-gatherers then heart disease would be a thing of the past. We also think of hardening of the arteries (so called calcification) as a problem of the elderly person with coronary artery disease, not seen commonly in middle aged individuals. So it is of great interest to see the publication of the HORUS study which has looked for evidence of vascular disease in 137 mummies from around the world (ancient Egypt, ancient Peru, the Ancestral Puebloans of southwest America and the Unangan of the Aleutian Islands). Using whole body CT scanning atherosclerosis was identifed by looking for the presence of calcified plaque in the wall of an artery. Atherosclerosis was noted in just over a third of mummies and in 4% of coronary arteries. This does not seem like a high proportion in the coronary arteries but we have to bear in mind that the average age of the mummies at death was 38 years. Although we commonly assume atherosclerosis to be a modern disease it was certainly present in pre-modern human beings and this raises significant questions about the basic predisposition and also the influences of lifestyle on the development of the atherosclerosis. Coronary artery disease. Sagittal 3D-volume rendered (A) and sagittal oblique 3D volume rendered (B) CT reconstruction of two mummies with coronary calcifications. (A) Coronary calcifications in the mummy of a Unangan woman (mummy 133) aged 47–51 years who lived in the late 19th century CE and was found on Kagamil Island of the Aleutian Islands. (B) Coronary artery calcifications in the mummy of Ahmose-Meritamun (mummy 35), an Egyptian princess aged 40–45 years who lived about 1580–1550 BCE and was found near modern day Luxor. RCA=right coronary artery. CE=common era. BCE=before common era 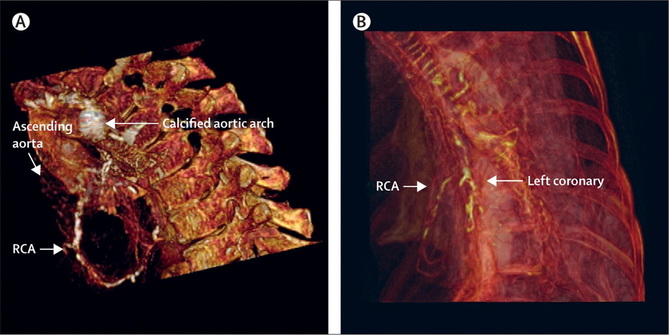
|

Dr Richard BogleThe opinions expressed in this blog are strictly those of the author and should not be construed as the opinion or policy of my employers nor recommendations for your care or anyone else's. Always seek professional guidance instead. Archives
August 2023
Categories
All

|
 RSS Feed
RSS Feed