BCIS Angioplasty Audit
All PCI procedures performed in the calendar year 2012 are included in this analysis. This excludes diagnostic angiograms, and pressure wire and intravascular ultrasound procedures unless they are associated with an angioplasty.
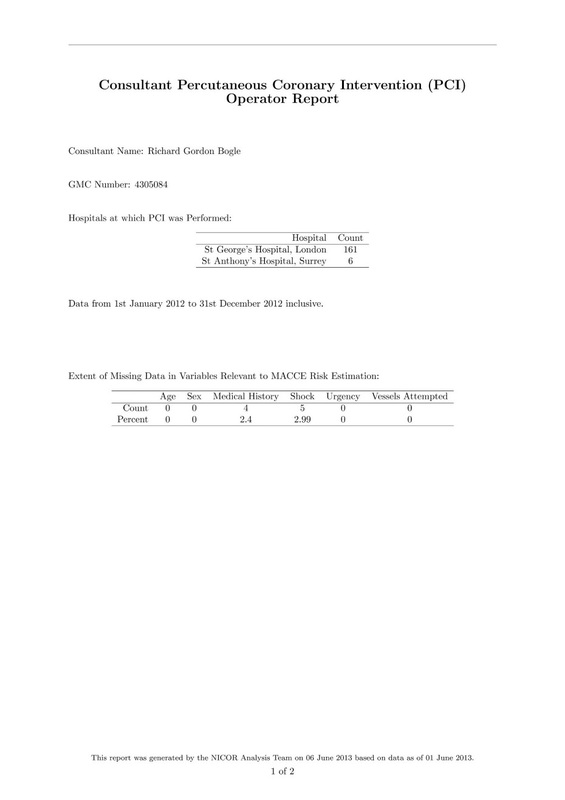
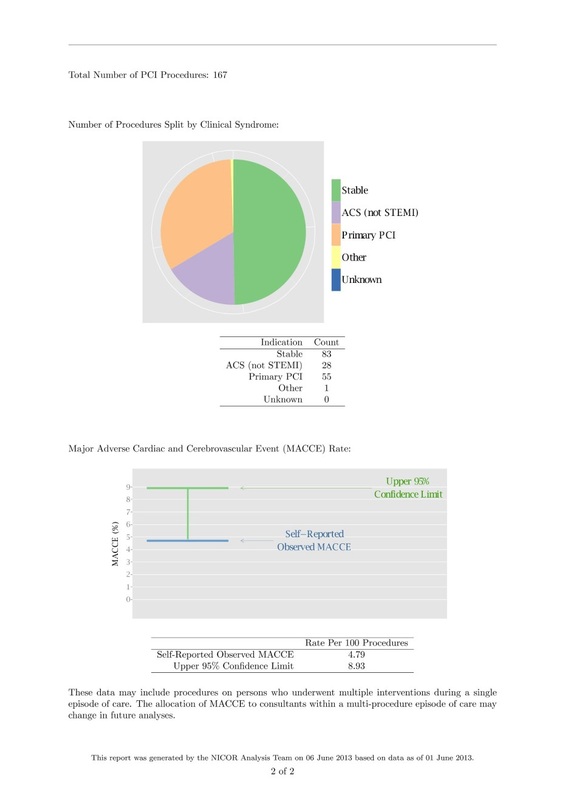
BCIS provide an analysis of: 1. Total number of PCI procedures performed by each operator, and the split by indication (such as stable, UA/NSTEMI and Primary PCI). 2. Risk adjusted MACCE (major adverse cardiovascular and cerebrovascular events). This includes the occurrence of any of the following up to the time of hospital discharge: death, the need for emergency cardiac surgery and stroke. In addition for those treated for stable angina it includes the development of a Q wave myocardial infarction. 3. Risk adjustment uses the Northwest Quality Improvement model, as has been used previously in BCIS audits to look at PCI centre risk adjusted outcome. Limitations are recognised by BCIS and work is underway on a 30 day mortality model which it is hoped will be used in the future. The analysis shown below was published on the BCIS website on 1st July 2013. Please note that I believe there are significant problems with the risk prediction model that BCIS have used to estimate the MACCE rate for individual operators. The MACCE rate of an operator will depend very much on the number of primary angioplasty procedures they perform for patients having a large heart attack. All of the deaths which occur in patients I performed angioplasty on in 2012 occurred in emergency patients undergoing primary PCI. You can review the data here and my individual data is shown below
|