Coronary angioplasty Andreas Gruentzig
The first coronary angioplasty was performed by Andreas Gruentzig in Zurich in September 1977. He had been working for many years on the idea that inflating a small balloon inside a narrowed coronary artery could relieve the obstruction to blood flow and treat patients with angina. Prior to that the only treatment was coronary artery bypass surgery which is a major open heart operation.
At first all of the balloon catheters used in angioplasty were handmade in a small shop in Zurich. The next major advance occured in the mid 1980's with the introduction of the first coronary stent and now 35 years later angioplasty or percutaneous coronary intervention (PCI), as it is commonly called, is a routine treatment in performed in most hospitals. Thousands of procedures are performed every day around the world and in the UK there were . During that time the size of the equipment used has become smaller, allowing PCI to be carried out via the radial artery in the wrist. The complexity of cases treated has increased and much of this has been assisted by the development of coronary stents which are metal scaffolds which hold the artery open after the balloon has dilated the narrowing. Stents have also helped to make angioplasty much safer and reduced the risk of needing emergency bypass surgery during an angioplasty. Coronary angioplasty is used in two situations. The first is in patients with a heart attack or unstable angina (chest pain at rest). Here there is strong evidence that treatment of a narrowed coronary artery, usually by dilatation with a balloon followed by implantation of a coronary stent, results in an improved prognosis, reduced risk of further heart attack and a lower likelihood of having further epsidoes of chest pain. The second situation is in people with stable angina (chest pain provoked with exercise in a predictable way) who also have a critical narrowing of a coronary artery. Here angioplasty is a good treatment for symptoms of chest pain although there is little evidence that it reduces the risk of heart attack or improves life expectancy. Sometimes people may have no chest pain but instead get short of breath on exercise and this may be due to a narrowed coronary artery. Again this can sometimes be helped with angioplasty. Other times people have virtually no symptoms but a narrowed coronary artery is discovered, for example, during a health screening assessment. Here if the artery is critically narrowed and there is evidence that it is resulting in lack of blood flow to the heart an angioplasty would be recommended. |

The shop in Zurich where the original balloon catheters were made.
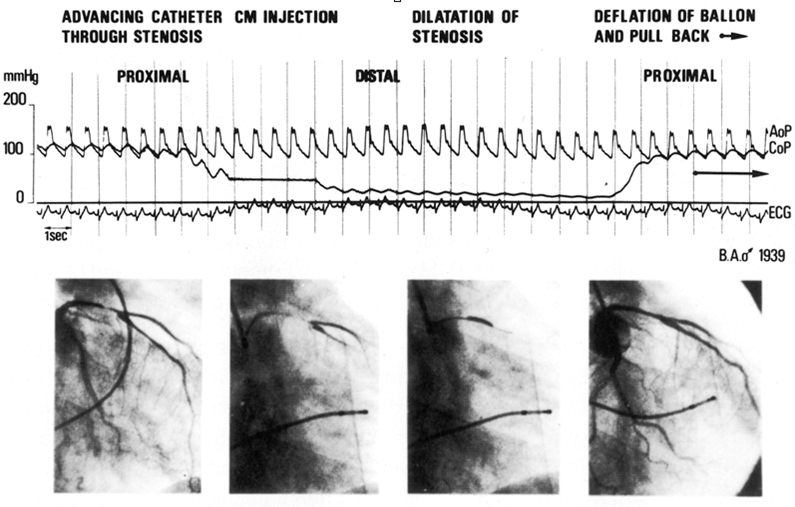
Pressure traces and angiogram images taken from the first cornary angioplaty procedure perfomed on 16h September 1977.
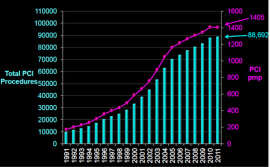
Number of PCI procedures and primary PCI procedures performed in the UK 1991-2011. Data from BCIS audit. www. bcis.org.uk
|
The angioplasty procedure
Below are some short videos illustrating what happens during an angioplasty procedure. They are for illustration only and procedures vary from patient to patient. In this example that angioplasty is performed via the femoral artery at the top of the leg. More commonly angioplasty is done via the radial artery in the wrist although this route may not be appropriate for every patient.
|
|
Patient preparationThis video clip shows the preparation in the catheter laboratory prior to an angioplast taking place.
An intravenous canula is place in a vein to administer medication such as a mild sedative. |
Equipment used in angioplastyThis film shows some of the equipment needed to perform angioplasty. The sheath is a small tube which is inserted into the femoral artery in groin or the radial artery in the wrist. The tube is between 1.3 and 1.8mm wide and 13cm long. Also shown are the balloon catheters and stents used to dilated the artery.
There are many different types of balloons and stent used to dilate coronary arteries. Most of the stents used are coated with a drug which reduces the chances that the artery will be come narrowed again at the site of the stent treatment. |
|
|
|
PCI procedureA coronary angiogram is taken at the start of the procedure to identify the area of narrowing. Following this a small, floppy guidewire is steered to the end of the coronary artery. Once the wire is in place a balloon catheter can be passed over the wire and then when it is at the site of the narrowing it is inflated. After thhis the stent, again mounted on a balloon catheter is positioned in the correct place and then deployed using a device called an indeflator.
Coronary stents are vary between 2.25mm and 5mm wide and the correct size is chosen depending on the size of the artery. Stents vary in length from 8mm through to as long as 38mm. More than one stent can be placed in the same artery. The stents are deployed into the artery at high pressure. This can often be at more than 12 atmospheres pressure. Just for reference the pressure inside your car's tyres is about 2-3 atmosphere! |
After the procedureThere is a period of recovery of several hours after the procedure. Some patients can go home the same day and others say for one night in the hospital.
Medication in the form of aspirin and clopidogrel is usually prescribed and it is very important that this is taken regularly after the procedure as it reduces the chances of problems occuring with the stent. Patients are also invited to take part in cardiac rehabilitation classes and exercise program which also reduces the risk of further heart problems from arising and contributes to well being and recovery. |
|