 When a patient has a coronary angiogram the cardiologist will report the results in terms of the degree of narrowing of the arteries. For example a 60% stenosis in the LAD, a 40% stenosis in the circumflex. But what does that really mean? Is the stenosis flow limiting? Is it responsible for the patients symptoms? Is the lesion prognostically significant? Should a stent be place? Is a bypass indicated? Many questions but the fundamental one is: "Would this patient's outcome be better with or without revascularisation or is medical therapy more appropriate?" When there is mild or critical coronary artery disease then the decision making is straightforward. However in many cases there are moderate areas of coronary narrowing. Showing the angiogram to several cardiologists will usually result in differing opinions about whether a lesion is flow limiting or not. For some cardiologists the "Oculostenotic reflex" is already potentiated leading to "iatrogenosis fulminans." In 1995 Steve Nissen and Eric Topol wrote about cardiologists preoccupation with luminography and eloquently showed how lesion assessment with angiography performed very poorly compared to intravascular ultrasound. They also wrote of the dissociation between the angiogram and clinical outcome and called for a shift in our with luminology towards measures that improve survival, freedom from myocardial infarction and symptoms of angina. Whether a coronary lesion is flow limiting is not just dependent on the degree of arterial stenosis but also on the amount of cardiac muscle supplied, the presence of collateral vessels, the length of the lesion and the function of the endothelium. Some of these factors can be assessed subjectively by angiography but others cannot. What is required is a more functional or physiological assessment. Cardiologists have fooled themselves for too long that they are able to determine the functional significance of a moderate coronary stenosis from the angiogram alone. Recent data using the pressure wire has challenged some of this thinking although there are still some sceptics. The FAME studies showed that use of the pressure wire to measure fractional flow reserve (FFR) could be useful to help in selecting the appropriate therapy and guiding coronary revascularization in patients referred for a percutaneous coronary intervention (PCI) procedure. Very recently a real world study has been published using FFR in patients referred for diagnostic angiography and looking at its impact on the decisions involved in revascularization. In this study patients referred for diagnostic angiography had a treatment plan for intermediate lesions (35-65% by eye) made on the basis of the angiography alone. 55% of patients were recommended to receive medical therapy and 45% revascularization (PCI, 38%; CABG, 7%). FFR measurement was then performed with the pressure wire and after this 58% of patients were recommended for medical therapy and 42% for revascularization (PCI, 32%; CABG, 10%). The results were not so different overall but in individual patients the FFR strategy changed the recommended treatment in 43% of cases. Reclassification was observed in 33% medical patients, 56% of PCI patients and 51% of CABG patients. These results are hugely important since they indicate that even experienced cardiologists are unable to judge the flow limiting nature of moderate lesions. In the initial medical treatment group one third of patients met FFR criteria for revascularisation. In the PCI group, half of patients were due to receive inappropriate or a less optimal type of revascularisation. In the surgical group over half of patients could have avoided an operation. What this study is telling us is that using the eyeball technique to judge the severity of coronary disease is not the best way to decide on a management plan for cardiac patients. If the practice of using a pressure wire became standard in diagnostic coronary angiograms it would lead to more patients receiving medical therapy, less receiving angioplasty and more patients having CABG. The effects on the economics of management of coronary disease are complex. Assuming everyone gets medical therapy then the cost of the increased CABG although a more expensive procedure is offset by the reduction in expenditure on angioplasty. The repeat revascularisation costs are likely to be lower since this has been shown routinely in most of the CABG versus PCI studies. There is of course the cost of the pressure wire for every case. Overall the most improtant thing is that the patient receives the most appropriate treatment and not at the mercy of the oculostenotic reflex. 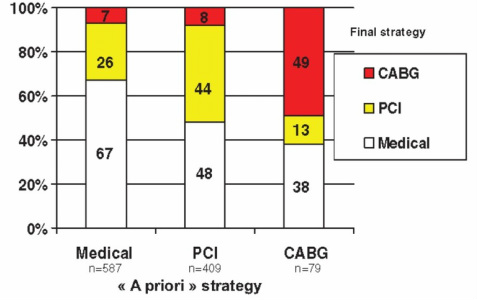
1 Comment
 Originally stable angina and acute myocardial infarction (MI) were believed to be different diseases. Then in the 1930s it was observed that some patients with severe and sometimes prolonged rest angina sometimes went on to have an MI. This disorder was referred to as pre-infarction or crescendo angina and then was renamed unstable angina in 1971. We still use this term today to describe a group of patients who have symptoms of angina at rest but who have normal cardiac biomarkers. The World Health Organization definition of MI requires 2 out of 3 of either typical symptoms of angina, a typical ECG pattern (e.g. Q waves, ST elevation) or a rise and fall in cardiac biomarkers of myocardial necrosis. In 1991 unstable angina was responsible for over half a million hospitalizations in the United States and it was one of the most common disorders leading to admission.
Nowadays we refer to patients with chest pain as having acute coronary syndromes. This term encompasses all patients with unstable angina, non-ST elevation MI and ST elevation MI under one umbrella. However there is ambiguity since the operational definition of unstable angina is made when there are new or worsening symptoms of ischemia and ischemic ECG changes with normal biomarkers. The distinction between new angina, worsening angina and unstable angina is clinically very difficult since by this definition the first ever episode of angina is unstable angina. The differentiation of unstable angina and MI now rests on the identification of abnormal levels of cardiac biomarkers. When I first started in medicine we measured serial CK, AST and LDH over 3 days and looked for the typical rise and fall in these biomarkers. Later we started using the more specific but not more sensitive CK-MB and finally we started to use to troponin. Troponin is a highly specific biomarker of cardiac muscle injury. The sensitivity of troponin is now so high that we are detecting elevated levels in many patients who had they presented to physicians 20 years ago were told they had not had an MI. In the TIMI3 trial a quarter of patients originally classified as having unstable angina based on CK-MB measurements had elevated Troponin and as the years have gone on the sensitivities of troponin assays continues to reduce. In the TIMI3 trial the cut point for MI diagnosis was 0.4ng/mL, by 2010 in the MERLIN-TIMI 36 trial the cut point was 0.04 ng/ml. In the recent PROTECT-TIMI 30 trial the cut point was 0.003ng/mL and in this trial 44% of patients were defined as having an MI at presentation with 82% by 8h. It is now evident that a large majority of patients with clinical manifestations of myocardial ischemia will have elevated levels of troponin if an assay with high enough sensitivity is used. What is also important is not just that we are detecting more MIs but this newly identified group of patients do have higher risk than those patients with undetectable troponin and as such aggressive treatment is leading to improved clinical outcomes. So in the end with ultra high sensitive troponin assays emerging into clinical practice we will be able to confidently divided patients into a group with stable angina pectoris and a group with MI and the grey zone of unstable angina with most likely be banished forever. |

Dr Richard BogleThe opinions expressed in this blog are strictly those of the author and should not be construed as the opinion or policy of my employers nor recommendations for your care or anyone else's. Always seek professional guidance instead. Archives
August 2023
Categories
All

|
 RSS Feed
RSS Feed