|
The ISCHAEMIA trial examined two approaches for the management of stable angina/ischaemic heart disease. The results have been much anticipated ever since the COURAGE trial shook the interventional community by showing that stenting in stable coronary artery disease was not associated with a reduction in cardiovascular events. The paper with the results of the ISCHAEMIA trial the results is not due out until next year but the results were been presented last weekend at the American Heart Association meeting in Philadelphia. Patients presenting with stable angina were assessed initially with a stress test. 75% had stress imaging test and 25% an exercise ECG. Subjects had to have evidence of ischaemia to be included in the trial (54% severe, 33% moderate and 12% mild ischaemia). Subjects also had a CT coronary angiogram to exclude left main stem disease (>50%) and to exclude people without CAD (<50% stenosis with stress imaging and <70% stenosis with exercise ECG). The results of the CT scan were not available to the clinicians – all they knew was the patient didn’t have left main disease and did have >50% in at least 1 major epicardial vessel. Patients were excluded if they had recent acute coronary syndrome, were highly symptomatic with angina, if eGFR <30ml/min or if the LVEF<35%. Subjects were randomised to either an invasive approach with cardiac catheterisation and revascularisation or a conservative approach with medical therapy. 5,179 patients were randomised (2,591 to conservative and 2,588 to invasive approach). Follow up was 4 years. The primary outcome was going to be CV Death and MI but this was changed in 2018 to a broader composite endpoint of CV death, MI, hospitalisation or unstable angina, heart failure or resuscitated cardiac arrest. Presumably this was because the event rate was smaller than expected. The prmary endpoint was not significant different between the two approaches. There was a significant increase in procedural MI (HR 2.98) and a significant decrease (HR 0.67) in non-procedural MI and admission to hospital with unstable angina (HR 0.5) in the invasive arm although the rates of all these events was low. The trial says that if you manage patients with angina, moderate-severe ischaemia and CT scan documented CAD by a conservative strategy you will not reduce the overall rate of CV events. If you choose a conservative strategy 9% of patients at 6 months and 28% at 4 years will end up having an angiogram, presumably due to symptoms, and 7% and 23% at 6 months and 4 years respectively will have revascularisation. If you choose an invasive approach about 2% of patients will have a procedural associated MI but there will be a reduced risk of non-procedural MI over the 4 years from about 10 to 8%. The risk of admission to hospital is reduced from from 2 to 1%. By any measure these are small effects. So was there a big difference in quality of life. The study used the Seattle Angina Questionnaire to assess the response to treatment. The probability of being angina free at 3 months was 45% if the subject had the invasive approach and had weekly symptoms of angina. For the conservative approach the chance of being angina free was just 15%. Care is needed in extrapolating these results beyond 3-months because the benefits of PCI usually reduce over time. Also we know ORBITA study there is a significant placebo effect of PCI procedures. If patients did not have angina there was no difference between the conservative and the invasice strategy. The Bottom Line for Patients: If you have stable angina, a positive stress test and no significant disease of the left main an angiogram/revascularisation will not your risk of having a major cardiovascular event in the next 4 years. If you opt for an invasive approach there is a small risk you will have a procedural related MI. This risk is balanced by a lower chance of being admitted with unstable angina or having a spontaneous MI. If you have moderate angina, then you have a higher likelihood of being free of angina if you have an invasive strategy versus a conservative strategy at 3 months, although the benefit may reduce over time. If you don't have angina there isn’t any tangible benefit of the invasive strategy and you should an invasive approach for the moment. The figure below is useful as it relates your baseline angina severity (x-axis) against the liklihood of being free of angina with the 2 approaches. 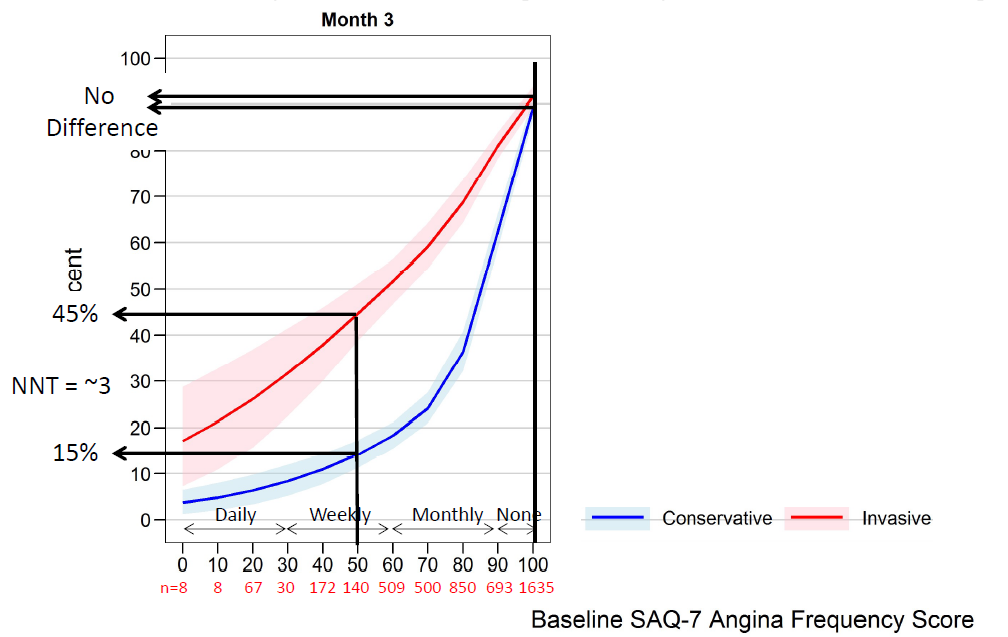 If you opt for a conservative approach there's a 1:3 chance you will end up with an angiogram in the 4 years and a 1:4 chance of having revascularisation due to symptom progression.
There will be a lot more discussion about the ISCHAEMIA trial as cardiologists and patients digest the results. The most important advice is don't rush to angiography and stenting for stable angina. Take time to consider the options. ischemia_main_11.15.19_final.pdf
0 Comments
|

Dr Richard BogleThe opinions expressed in this blog are strictly those of the author and should not be construed as the opinion or policy of my employers nor recommendations for your care or anyone else's. Always seek professional guidance instead. Archives
August 2023
Categories
All

|
 RSS Feed
RSS Feed