 When patients come to a hospital outpatient clinic it is common for them to be asked about the medication they are taking. As a physician, medicines are your main weapon against disease and even as an interventional cardiologist I spend most of my time intervening with my pen rather than with catheters. It is essential for the doctor to know which medication the patient is taking and in what dose. Some patient with angina, high blood pressure or diabetes are prescribed over 10 different medications, but how many of them are being taken?
Compliance is understood to mean acting in accordance with advice of the prescriber. The word is linked with an old-fashioned paternalistic attitudes towards the patient by the prescriber and so instead the idea of concordance, implying that prescriber and patient were in general agreement about the drug regimen is preferred. Some people prefer the term adherence which implies a steady observance or maintenance. So in the clinic how do we really know whether our patients are adhering to their medications as prescribed? A study just published in Heart looked at this question in 208 patients referred their secondary care hypertension clinic. Using an HPLC assay to detect 40 of the most commonly prescribed antihypertensive medications they ran samples of the patient's urine to see if the drugs on prescription chart were present in the urine. Shockingly in 25% of patients only some of the blood pressure medications were found and in 10% none were found. This follows on from a study in Germany that looked at 108 patients with resistant hypertension. Of these 15 patients had secondary causes of hypertension and 17 achieved blood pressure control by the addition another drug. In the remaining 76 patients, using the same type of HPLC analysis of the urine, 53% of patients were non-adherent to the prescribed medication and 30% were not taking any blood pressure medication at all. Patients with resistant hypertension are often sent for expensive investigations such as MRIs, blood and urine tests looking for secondary hypertension often with normal results. Apart from higher BP levels and elevated heart rate, adherent and non-adherent patients are indistinguishable which supports the idea that a doctors impression, patient's interviews or pill counts are not reliable markers of adherence. With the results from these studies in mind a formal check of adherence to treatment using a urine analysis would be helpful. Of course this can't give the whole picture since it is also recognised that patients adherence to treatments increases around the time of clinic appointments. In the future it is likely that we will be able to monitor medication adherence. New smart pills containing a silicon chip the size of a grain of sand are already a reality. Composed of trace amounts of magnesium and copper, when swallowed, they react with stomach acid generating a tiny voltage which can be detected by a special skin patch and relayed to a smartphone. These can be built into a medication and would allow doctors to know if medication has been taken and also act as a remind to the patient who might have forgotten to take their tablets. With some medicines such as the new oral anticoagulants addition of this technology could be very cost effective as improved adherence is very likely to improve patient outcomes.
0 Comments
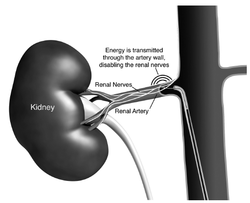 In December 2009 The Telegraph ran an article describing a revolutionary new procedure which was aimed to be able to effectively cure high blood pressure. Like many people I was excited to find out more. A clinical trial been published in April 2009 in the Lancet describing the effects of destroying the nerves which supply the kidneys in 50 patients with resistant hypertension. This observational study had shown impressive and sustained blood-pressure reduction without serious adverse events. Following that a randomised clinical trial of 110 patients was started and the Telegraph article was prompted by the first patient in the UK being treated at the London Chest Hospital as part of the trial. When the study was finally published in December 2010 again it showed impressive and sustained reductions in blood pressure. These results stimulated excitement amongst interventional cardiologists who wanted access to this new treatment for their patients. Research was quoted by experts in the field estimating that there were huge numbers of patients with resistant hypertension for whom this therapy was potentially an option. Ardian, the company which made the ablation catheter, was valued at 800 million dollars and rapidly acquired by Medtronic one of the largest medical device companies in the world.
Ablation devices were rapidly and widely promoted in Europe. Courses and international meetings were established by proponents of the device and sponsored by the device company. Reputations and CVs of the organisers and speakers were enhanced and by August 2012 it was though that over 5000 procedures had been performed. In particular German cardiologists embraced the technology with hundreds of patients being treated. Enthusiasm spread and papers started to appear proposing that renal denervation might be a potential treatment for metabolic syndrome, type 2 diabetes, sleep apnoea and heart failure. Much of this based on uncontrolled studies in a few highly selected patients. It all seemed to good to be true. UK cardiologists, including myself, started to work out how they could begin to perform this novel procedure. Interventional cardiologists like technology and the prospect of being able to perform a new procedure was very attractive. In many cases charitable funding was raised to purchase the catheters and ablation system. Collaborations were established between radiologists, hypertension experts and cardiologists, a NICE technology appraisal was published, followed by guidelines from the British Hypertension Society and the prospect of "Commission by Evaluation" from NHS England. Centres, including my own at St Helier Hospital in Carshalton, started to perform the procedure in small numbers. Our initial enthusiasm for the procedure was tempered by a difficulty in finding the apparently huge number of patients we were told had resistant hypertension. We were referred many patients for evaluation but usually simple medication adjustment such as the addition of spironolactone or treatment of other factors such as sleep apnoea were able to control the blood pressure. Sometimes patients simply had white coat hypertension and proper assessment with ambulatory monitoring revealed well controlled blood pressure. Sometimes the patient did have resistant hypertension but the renal artery anatomy wasn't suitable for ablation. Overall only about 1 in 10 patients we screened were suitable and we started to think that the epidemic of resistant hypertension (defined in guidelines as BP>140mmHg on 3 drugs including a diuretic but for the purposes of the denervation trials a BP threshold of >160mmHg was required) did not really exist. In the USA things were a little different. The Food and Drug Administration (FDA) concluded that the clinical trials which Ardian had performed were not adequate for licencing the technology since there was no sham treated group. Without this it is possible that significant bias has crept into the trials especially when the end point being measured was office blood pressure. The FDA required a double blind, sham controlled trial and we all awaited eagerly for the results. This week our wait ended earlier than expected when Medtronic put out a press release to say that their pivotal trial had failed to meet its primary efficacy endpoint. In other words there was no difference in the office blood pressure measurement from baseline to 6 months in patients treated with the ablation versus sham treated patients. Fortunately no safety concerns were raised from the trial. The data and full results have not been published yet and so it is difficult to comment in detail but at this stage it is certainly very disappointing that the blood pressure effects seen previously were not reproduced in a sham controlled double blind clinical trial. There are two lessons here. First, the placebo effect and bias are strong factors which influence clinical outcomes. The bigger the procedure, the more invasive it is and the more enthusiastic the doctor the greater is the chance of a very significant placebo effect. The only way to avoid this is a sham or placebo controlled trial. Second, it is often said that history repeats itself and there are parallels here with renal artery angioplasty. This procedure started in the 1970s with case series suggesting it reduced blood pressure in everybody with renal artery stenosis. The first randomized trial was published in 1998 and since then all the trials comparing medical treatment with renal angioplasty were negative. So where does that leave us with renal denervation. It's early days but we should be cautious and I think that in general renal denervation should now only be performed as part of blinded sham controlled research clinical trials.  For hundreds of thousands of years, humans evolved on a diet that contained just a trace of salt. The Yanomamo Indians of the Amazon basin were first studied by Western society in the 1950s and provide an insight into what happens to blood pressure when salt consumption is extremely low. In the 1950's the Yanomamo were consuming a primative diet that contained <1g of salt a day. The most striking feature of this diet was that the blood pressure in the older Yanomamo was the same as that in the adolescents. Salt is ubiquitous in food with 75% of daily salt intake hidden in processed food. There is abundant evidence from clinical trials indicating that a usual salt intake (3-4.5g per day) has adverse effects on the heart and blood vessels. A high salt diet predisposes to high blood pressure which leads to stroke and heart failure. A recent study looked at 17 mildly hypertensive adults randomised to 4 weeks of reduced (1.2-1.5g) or usual (3.6g) salt intake. BP pressure fell by 12mmHg and vascular function improved in subjects receiving the low salt diet. In this study the reduction in blood pressure caused by reducing salt intake is similar to the amount normally achieved by blood pressure medication. It would be difficut to follow a Yanomamo diet but dietary salt reduction is possible by following the DASH (Dietary Approaches to Stop Hypertension) diet which reduces salt intake by about 50%. Implimentation of low salt diets requires action by politicians, food companies and retailers, as well as consumers. If salt intake could be reduced by 50% it is estimated that in the USA this would lead to 90,000 fewer heart attacks, 48,000 fewer strokes and save $18 billion each year. We have known about the associaion between salt intake and blood pressure for many years and the evidence is growing to support a reduction in salt consumption to bring about positive health benefits. Pressure groups such as the Consensus Action on Salt and Health are trying to persuade all stakeholders to reduce salt and have made some important progress. Watch out for Salt Awareness Week (11-17th March 2013).  Jablonski KL. Racine ML. Geolfos CJ. Gates PE. Chonchol M. McQueen MB. Seals DS.
Dietary Sodium Restriction Reverses Vascular Endothelial Dysfunction in Middle-Aged/Older Adults With Moderately Elevated Systolic Blood Pressure J Am Coll Cardiol. 2013;61(3):335-343. doi:10.1016/j.jacc.2012.09.010 Oliver WJ. Cohen EL and Neel JV. Blood pressure, sodium intake, and sodium related hormones in the Yanomamo Indians, a "no-salt" culture. Circulation. 1975 Jul;52(1):146-51. |

Dr Richard BogleThe opinions expressed in this blog are strictly those of the author and should not be construed as the opinion or policy of my employers nor recommendations for your care or anyone else's. Always seek professional guidance instead. Archives
August 2023
Categories
All

|
 RSS Feed
RSS Feed