 20 years ago today two pivotal papers were published in the New England Journal of Medicine. The BENESTENT and the Stent Restenosis Study compared balloon angioplasty to coronary stenting in people with stable angina. What people remember is that stents were superior to balloons and the rest as they say is history. But the story is more complex than that as the trials show. Stents had been around since the late 1980's and they were effective in treating acute vessel closure due to balloon-induced dissection. This complication was the Achilles heel of interventional cardiology and led patients to emergency bypass grafting when their coronary artery closed off during or shortly after the procedure. Unfortunately Achilles had two heels and the other one was restenosis. Some people thought that stents might be useful to reduce the rate of restenosis but there was a problem. Stents were metal which required use of combinations of aspirin, dipyridamole, heparin and then for three months warfarin. This therapy exposed the patient to a risk of major bleeding and vascular complications prolonging hospital stay. In those days vascular access was via the femoral artery and the sheaths were about 3mm wide. Read today the results of the trials are interesting. Take the BENESTENT trial, the rate of in-hospital events was similar in both groups (6.2% in the balloon vs. 6.9% in the stent group). There was no difference in the incidence of myocardial infarction or in the need for urgent or elective cardiac surgery or second angioplasty during the hospital stay. Stent thrombosis occurred in 3.5% and subacute vessel closure after balloon angioplasty in 2.7%. The incidence of bleeding and vascular complications was 4 times higher at 13.5% after stent implantation than after balloon angioplasty. Hospital stay was 8.5 days after a stent and 3.1 days after a balloon. Now reading this is I am surprised. Stents were not so much better than plain old balloon angioplasty. Acute vessel occlusion was swapped for stent thrombosis and because of the anticoagulation patients had more complications and stayed much longer in hospital. There was no early gain. 20 years on an a coronary stent is a day case procedure done through a tube less than 2mm wide via the wrist and with a complication rate less than 1% and re-stenosis rates almost as low. The requirement for on site surgery is a thing of the past. The speciality of interventional cardiology is now mature. Where will it be in another 20 years?
0 Comments
In 1958 Mason Sones famously, and apparently accidentally, performed the first coronary angiogram at the Cleveland Clinic. From then on much of the clinical care of patients with ischaemic heart disease was based on research that relied heavily on the visual interpretation of the coronary angiogram. However it wasn't long before papers stared to appear which questioned the accuracy and reproducibility of these visual estimates. One paper from 1976 reported than nearly half the time a group of experienced cardiologists could not agree on the presence of significant coronary artery disease. Other studies followed alleging to to demonstrate the benefits of performing quantitative coronary angiography using computers to assist in the measurement of the degree of narrowing. These methods were more reproducible than eyeballing the angiogram but still there was disagreement and the methodology was time consuming. Take for example this angiogram on shown below. Do you think the this LAD stenosis is flow limiting? Why not vote here and see what others think?
By early 1990's the literature on the accuracy of angiogram went quiet. Cardiologists had other things on their mind - namely coronary angioplasty and stenting. Angiography was the test which fuelled the fire of angioplasty and so the problems with assessment of flow limiting lesions and lesion significance drifted into the background. The occulo-stenostic reflex was strong. Cardiologists needed their angiograms too much to call into question the ability of the test to diagnose and classify the severity of the coronary lesions. This was the era of eminence-based medicine when expert opinion trumped anything else. The poor reproducibility and difficulty in assessment of lesion was forgotten.
When you learn angiography you quickly realise that the interpretation is difficult. When you work for a number of bosses you start to see a difference in their practice. Some always see a moderate lesion as severe, or a severe lesion as critical. The phrase "the angiogram often underestimates the severity of disease" is often be heard in the catheter lab control room as the guide catheter is being opened ready for angioplasty. Whilst there is usually agreement about the mild (<30%) and severe (>80%) lesions it is the moderate ones which are most difficult and unfortunately most common. As I teach my fellows the percent stenosis is the wrong way to think about lesions, rather we should say whether we believe a lesion to be flow limiting or not. Flow limitation is dependent on the stenosis but also on the reference vessel size, the lesion length, the size of the territory supplied by the vessel and the presence or absence of collaterals. The issue of interpretation is vital to the individual patient since it determines what treatment is recommended, You don't want a cardiologist to put in a stent or offer bypass surgery if your coronary artery lesion is not flow limiting. Recent studies have revealed what we knew all along namely that when coronary artery disease is moderate it is not possible to accurately know by visual assessment whether the lesion(s) are flow limiting or not. We need better methods not based on anatomy but rather on physiology. I have previously written about the RIPCORD trial but recently a large French registry has published its results which support the idea that the angiogram is difficult to interpret and that use of a pressure wire to measure fractional flow reserve (FFR) alters the cardiologists decision making. The R3F study looked at 1000 people having a diagnostic angiogram. The vessels were assessed and significant lesions documented. The patients symptoms and the results of any non-invasive investigations were considered and a recommendation made as to whether the patient should have medical therapy, angioplasty or bypass surgery. After this the cardiologists performed a pressure wire measurement (FFR) of any stenosis. The results were then used to determine whether the stenosis was flow limiting and with this information in hand the treatment recommendation adjusted. So for example if a patient had a 40% stenosis on the angiogram with medical therapy recommended initially but then the pressure wire was significant (e.g. FFR 0.74) the recommended treatment would be to offer an angioplasty. Using the pressure wire data the overall number of people recommended for medical therapy, angioplasty or bypass did not change but the decision for an individual patient changed 43% of the time. Overall the decision changed in 33% of patients initially recommended to have medical therapy and 50% of patients recommended to have angioplasty or bypass surgery. These results are very important for individual patients since the treatment recommendation means the difference between just taking tablets versus having a procedure or an operation. We don't know yet whether a pressure wire guided approach makes a difference to clinical endpoints such as survival, mortality, rates of heart attacks and a large trial is needed to answer this question. For the moment when a moderate stenosis is diagnosed the patient should be asking their cardiologist what is the FFR? How good are cardiologists at assessing the significance of a coronary narrowing on an angiogram. If your cardiologist tells you that your artery is 95% narrowed is that really true? A 3mm vessel narrowed by 95% means the lumen size is only 0.15mm wide. That's very small - smaller in fact than a standard angioplasty guide-wire (0.36mm) and so the wire should occlude the artery when it crosses the lesion - this rarely happens. Precise assessments of severity of coronary stenosis by angiography are unreliable. But how unreliable? Patients and cardiologists are fixated on the degree of coronary stenosis. Tell a patient his artery is 50% narrow he is worried, tell him it's 90% narrowed his is beside himself - it could block off at any time he thinks. Is a patient with a 60% stenosis in less trouble than someone with an 80% one? Rather than becoming fixated about the percentage stenosis of an artery I prefer to grade lesions as significant or non-significant. Significant lesions cause limitation of blood flow during exercise or stress, non-significant ones don't. Patients with significant lesions may have improved quality of life/symptoms improved by local lesion treatment with a stent or coronary bypass. Patients with non-significant lesions are better off with medical therapy and should avoid stents or bypass as they are unlikely to be beneficial. The discussions of significance require cardiologists to transform anatomical data derived from an angiogram into functional data which is dependent on length of lesion, severity of stenosis, presence of collaterals etc. When lesions are very severe or very mild cardiologists will agree when asked to grade the severity. When arteries are moderately diseased the agreement turns to disagreement. What we need is a functional assessment of lesion significance. This can be provided by pre-angiography investigation with tests such as nuclear perfusion imaging and stress echocardiography giving information about regional ischaemia. But NICE says we should move to angiography when the risk of underlying coronary artery disease is more than 60% and so often patients find themselves having an invasive angiogram as the first line investigation in the absence of any information about coronary ischaemia. 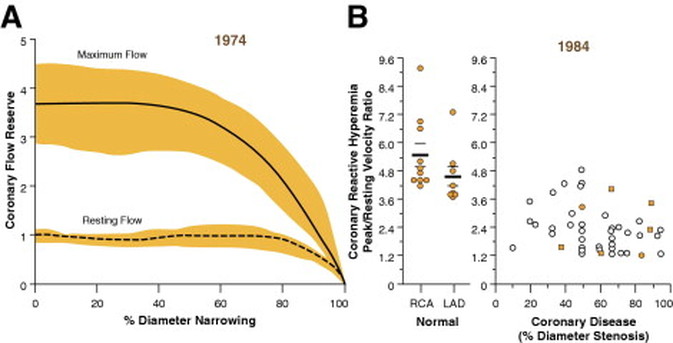 This week sees the publication of the RIPCORD trial which is a UK based study which looked at the role of pressure wire assessment to guide therapy of coronary artery disease. The group took 200 patients with angina and performed coronary angiography. A cardiologist formulated a management plan of either medical therapy, angioplasty, bypass surgery or unable to make a decision with further information required. At that point a second cardiologist came in an performed an FFR measurement with a pressure wire. After this the results were shared with the first cardiologist to see whether this altered the management plan for the patient.
The good news is that 74% of the time the management plan didn't change after the FFR measurement. In 72 patients medical treatment was recommended. In 9 patients revascularization was recommended after the FFR test (6 PCI, 3 CABG). In contrast, 25 patients who had been recommended for revascularization after angiogram (24 PCI, 1 CABG) were switched to medical therapy after the FFR data became available. In the total group of 200 cases after an angiogram 90 were led to the recommendation of PCI to ≥1 vessel, but in 24 (26.7%) there was no physiologically significant stenosis detected by FFR. So a quarter of patients recommended for an angioplasty did not have evidence of flow limiting disease and therefore the procedure would have been potentially worthless. So what does all this mean. First cardiologists can predict lesion significance from an angiogram in about 75% of cases. In fact that is not bad an it would be very interesting to see in this study if some cardiologists were better than others at making this prediction. My guess is there would be. Second it means that we are recommending some patients to have medical therapy when they would be benefit from revascularisation and we are subjecting some patients to invasive or surgical treatments without any reliable evidence that their coronary arteries are significantly narrowed. An approach to use the FFR measurement more widely gets the right treatment for the right patient. But this comes at a cost of about £450 extra per case because the pressure wire adds an expense to the angiogram. Second the complication rate from an FFR procedure is higher than that of diagnostic angiography and some patients with non-flow limiting lesions may sustain a complication such as coronary dissection which requires emergency surgery or stenting. Overall we should move to a more accurate way of diagnosing coronary artery disease and being able to assess lesions in detail at the time of angiography is likely to gain momentum. Cardiologists need to stop kidding themselves and their patients that they can assess the significance of a coronary stenosis accurately every time.  In the Summer of 2012 David Brailsford presided over Team GB’s incredible haul of cycling medals in the Olympic games. What was the secret of this team’s success? The simple answer was there wasn’t one secret but as Dave Brailsford said it was the aggregation of marginal gains. Performing a coronary angioplasty can take as little as 15 minutes but even with the simplest procedure there are many different choices which the operator needs to make and each of these influences the outcome of the procedure and the risk of complications. Close attention to detail, wise choices and the sum of the marginal gains makes the difference between getting a bronze and achieving gold.
Here is an example. The patient is a 75 year old obese man with diabetes and hypertension. He has a stenosis in the mid right coronary artery. The artery is mildly calcified and a somewhat tortuous. Dr Groin is a default femoral operator. With a 6F sheath, a right Judkin’s guide catheter and a hydrophilic guide wire most cases can be done. Groin access takes but a moment and the coronary artery is easily intubated, the wire glides through the vessel with its usual speed and hydrophilic coating. Within moments the lesion is pre-dilated with a balloon. Then comes the stent but there is a problem, the tortuousity and the calcification makes the stent difficult to track through the vessel. The JR4 catheter does not give any support and the stent cannot be manoeuvred into the correct place. A buddy wire is passed but still the stent won’t track to the lesion. Further ballooning is performed in the vessel which results in a small dissection and without the ability to deliver a drug coated stent they try a bare metal stent which is finally deployed with a reasonable result. The procedure takes 75 minutes and there is 300ml contrast used. An angioseal vascular closure device is deployed but does not quite seal the artery completely and the patient develops a haematoma. The patient eventually leaves the hospital 4 days later. His procedure was a success, the vessel was stented but was this as good as it could possibly be. Dr Wrist usually takes the radial approach. A 5Fglideliner sheath and a 6F AL1 guide catheter are used because the vessel is calcified and somewhat tortuous and he thinks that extra support may be needed. The lesion is crossed with a supportive angioplasty wire, the wire is harder to manipulate than the hydrophilic coated wires but once in the distal vessel it gives excellent support and remains very stable. The vessel is tortuous but the AL-1 gives a really good back up support and the lesion is ballooned with a 2.5x12 balloon and then a 3.5x15 drug eluting stent is deployed with a good result. Because the lesion was calcified a further 3.5x12 non-compliant balloon inflation is made to high pressure with a very good angiographic result. The procedure takes 27 minutes and there is 60ml contrast used. A TR band is placed on the wrist with patent haemostasis and the patient is discharged from the hospital 6h later. His procedure was a success, the vessel was stented. Both patients had a successful PCI on paper but Dr Wrist’s procedure was more successful for the patient. The sum of the small parts – access site, catheter choice, wire choice and ability to deliver devices. All of these single decisions feed into the outcome of the procedure for the patient. Alone each one of these things may contribute only a fraction of a percent to a difference in outcome but when they are all put together they can add up and the sum of marginal gains leads to safer and more effective practice. So how do we achieve these marginal gains in practice: Set audacious goals, work with others who share your vision. Focus, Focus, Focus. Collect high quality procedure data, outcomes data and learn from it. Be disciplined to capture every gain. 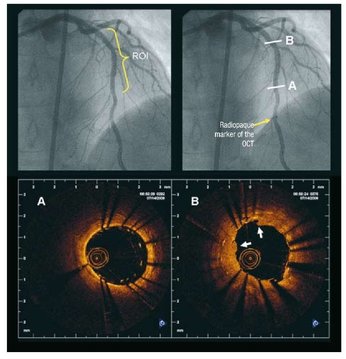 Angiography of the LAD artery & optical coherence tomography Angiography of the LAD artery & optical coherence tomography The universal approach for deployment of a coronary stents is to use high pressure inflations. This is because high-pressure improves stent expansion and apposition and markedly decreases the incidence of acute and subacute stent thrombosis.
In contrast there is no standard protocol for the duration of the high-pressure inflation. Often when a stent is placed the inflation pressure tends to gradually decrease over time suggesting that there is on going slow stent expansion. If the stent further expands with the same inflation pressure then a rapid inflation/deflation sequence may not adequately expand the stent even if the final angiogram looks good. It is possible that sustained inflation until pressure stabilizes would result in more optimal stent deployment. The possibility of incomplete strut apposition may also be heightened if inadequate time is allowed for stent expansion. A recent study has looked at 12 patients having single vessel stent interventions using the new technique of optical coherence tomography. This is an ultrasensitive method that can visualise the apposition of individual stent struts. After pre-dilation the lesions were stented with no angiographic residual stenosis after high-pressure stent balloon inflation of relatively short duration (“rapid” inflation) with an average inflation time of 28±17 sec. Following an OCT measurement prolonged inflation was performed. The inflation time was chosen such that the pressure in the inflation device was completely stable for at least 30 seconds. In order to achieve this it required much longer periods of inflation for 206 ± 115 sec. The patients appeared to be stable during this long inflation but what is interesting is that the minimal stent diameter and minimal stent area both increased after prolonged inflation compared with rapid inflation. Stent diameter increased by 9% from 2.75 ± 0.44 to 3.0 ± 0.5 (P < 0.0001) and stent area by 18% from 6.63 ± 1.85 to 7.83 ± 2.45. Not only this but stent strut mal-apposition was halved. This is a small study but important as it makes us think once again that the coronary angiographic results is a relatively crude guide to the apposition of the struts and the overall deployment of a stent. We should consider using both high pressure and longer inflations. |

Dr Richard BogleThe opinions expressed in this blog are strictly those of the author and should not be construed as the opinion or policy of my employers nor recommendations for your care or anyone else's. Always seek professional guidance instead. Archives
August 2023
Categories
All

|

 RSS Feed
RSS Feed