 In 1975 a simple ceremony was held at the Horton Hospital in Epsom. A plaque was unvieled commemorating the contribution made between 1925 and 1965 towards the "relief of suffering". The building housed the Mott Clinic also known as the Horton Malaria Laboratory. It was here, before the discovery of penicillin, that malaria infected mosquitos were used to treat patients with syphilis. In Vienna at the end of world war one Professor Wagner-Jauregg dicovered that malaria-induced fever was effective in the treatment of the syphilitic condiiton General Paralysis of the Insane (GPI). GPI was a serious problem affecting about 10% of patients in psychiatric hospitals and there was until that time no effective treatment. The malaria therapy was reported to result in over 80% of patients were free of disease progression. The treatment was introduced rapidly into England but there was lack of awareness of the lethal effects of certain species of human malaria parasites such as Plasmodium falciparum. Horton was chosen to treat these patients because after a pilot study at Cane Hill and Claybury hospitals they found that there was a high risk that malaria would spread between patients; Horton was ideal because of the fourteen bed isolation hospital and so to try and render the treatment as safe as possible the Mott Clinic and Horton Laboratory was established. Colonel S. P. James, was the first director and he found a strain of malaria in Madagasca that was safe for use in man. In May 1925, mosquitoes infected with this strain were taken to Horton and fed on two female patients.The function of the laboratory was to provide malaria parasites use in the treatment of GPI and this continued until penicillin made the treatment obsolete. Overall the clinic provided treatment for thousands of patients sufferering from GPI with more than 16,000 treated in Horton Hospital itself. A stream of publications appeared in scientific journals originating from the Horton Laboratory including the discovery of the exoerythrocytic parasite in the liver in man in 1948. The laboratory moved into the testing synthetic antimalarial drugs in conditions of maximum secrecy during the second world war. The laboratory closed in 1973 and its memorabilia and archives are held at the Wellcome Museum and the London School of Hygiene and Tropical Medicine. Epsom and Ewell Archives 
Aerial view of Horton Hospital
0 Comments
 The debate over whether patients with 3 vessel coronary artery disease should be treated with multi-vessel stenting (PCI) or coronary bypass surgery (CABG) has raged for the last decade. Stenting only needed to be as good as surgery for it to become the treatment of choice since the procedure is less invasive and the recovery time quicker. Comparison of the two forms of treatment has been difficult because stents have been constantly improved meaning that every trial was out of date compared to currently available technology at the time the results were published. This week the final 5 year results of the SYNTAX trial were published in the Lancet. This trial randomised 1800 patients to stents or surgery. The average age of the patients was 65 years, 75% were men and 25% diabetic. The combined end point included all-cause mortality, stroke, myocardial infarction and repeat revascularisation. The results showed that 26·9% in the CABG group and 37·3% in the PCI group reached that endpoint (p<0·0001). Myocardial infarction was higher in the PCI group (9.7% vs 3·8%; p<0·0001), as was the need for repeat revascularisation (25·9% vs 13.7%; p<0·0001). All-cause death and stroke were not different.
So what can we learn from this trial. First the CABG group appear to get continued benefit as time went on. One explanation for this is that since CABG bypasses, any disease progressing in the artery proximal to the insertion point of the bypass graft remains treated which is not the case if a stent has been implanted. This may not be the whole explanation since CABG did not show a benefit over PCI in the left main stem treatment group although there were only 222 patients in this group. Second, SYNTAX acknowledged that not all 3 vessel disease is the same with some patients have discrete, simple lesions and others having very complex disease. Embedded in this trial was a scoring system (www.syntaxscore.com) which allowed a measure of the severity of the coronary artery disease. Treatment of low score (22 or less) or an isolated left main stem stenosis with CABG did not appear to confer an advantage over stents. In contrast an intermediate or high SYNTAX score predicted a significantly worse outcome if treated with stents rather than CABG. The results indicate that patients with simple three vessel disease could reasonably be treated with stents rather than surgery although it is important to remember that the analysis of subgroups in clinical trials is only hypothesis generating. The subgroups do not have enough patients in them to be adequately powered to draw definitive conclusions. Calculation of the SYNTAX Score gives the cardiologist an estimate of the severity of disease and helps feed into the decision making process regarding the best means of revascularisation. The other issue is that of patient choice. More patients randomised to CABG withdrew from the trial compared to PCI. Faced with a decision regarding what treatment to have the patient will have views and these need to be informed by a discussion of the best available evidence. If a patient understands that stents may have a less good outcome they may still decide to have this treatment because it is less invasive than CABG. The SYNTAX trial also leaves open the question of how to manage much older patients where the risk of stroke and mortality is greater. Many patients we currently see are in their late 70s or 80s, often with severe coronary disease and they may be less included to undergo CABG. Also most of the participants in SYNTAX were male and therefore it is difficult to know whether the outcomes for women would be the same. The SYNTAX trial is an important landmark to inform how we should manage severe coronary artery disease. However we need to remember that as cardiologists we treat individual people and the results of the clinical trials present results from pooled groups of patients may not always be representative of the patient in front of us. Coronary artery bypass graft surgery versus percutaneous coronary intervention in patients with three-vessel disease and left main coronary disease: 5-year follow-up of the randomised, clinical SYNTAX trial  When a person has a heart attack they often ask why it happened? This is a normal reaction because if you understand why an illness occured then it might be possible to take action to prevent it from occurring again or progressing. Apart from the traditional cardiac risk factors such as age, male gender, smoking, high blood pressure, diabetes and high cholesterol, patients often ask me if job stress has been involved.
The Whitehall study performed in the 1980s showed that chronic work stress was associated with increased risk of coronary heart disease especially in men under 50 years old. This was also seen in the INTERHEART study which found that stress at work was associated with more than twice the risk of heart attack. The Womens Health Study also confirmed that the effect of stress on heart disease was not limited to men. Last October The Lancet published a large, individual patient-level meta-analysis of 197473 European men and women without pre-existing coronary heart disease to try and investigate the effect of job strain on development of coronary heart disease. In the study 15% of partipants reported job strain which might be seen as a relatively low overall level of stress. The study assessed both the demands placed on the workers and the degree of control they had over their work. Four groups were identified. Low job strain (low demands/high control), passive (low demands/low control), active (high demands/high control) and high strain (high demands/low control). Compared to the low job strain group, the high control/high demands group did not have increased risk of coornary heart disease. In contrast those workers with low demand/low control jobs had increased risk and the risk was even higher in those with doing jobs with high demands and low control. These results indicate that it is the degree of control a worker has over the demands placed on him or her that determines whether the job increases the risk of coronary disease. A high work pace is not necessarily a stressor if the worker has control. A difficult task might be seen as a challenge rather than being excessively strenuous. Much of this work was carried out in industrial settings and the modern world of work is different and other factors such as the effort-reward imbalance model and job insecurity are likely to be of major importance in the future. So when a person asks: Did stress cause my heart attack? More than a simple yes or no answer is required. You need to understand what job they have been doing and at what level. Getting an idea of the degree of control the individual had to regulate the demands of the job is critical in understanding the role of stress in heart disease. Job Strain and Coronary Heart Disease - Lancet Whitehall Study - Stress & Health Study Job Strain, Job Insecurity, and Incident Cardiovascular Disease in the Women’s Health Study: Results from a 10-Year Prospective Study INTERHEART Study  Every day about 400 millions searches are done using the Google search engine. Many of these searches are looking for health information and for every one the search terms, location of the computer and the time of search are stored. This data can be explored freely using Google Trends but can these trends tell us anything useful about disease patterns and do they have any potential to improve healthcare?
 When a patient is admitted to St George's Hospital for a daycase cardiac procedure the chances are they will spend part of the day on James Hope Ward. Situated on the first floor of Atkinson Morley Wing this busy ward sees a constant stream of patients admitted for coronary angiograms, angioplasty or cardioversion. Whilst recovering they might wonder who was James Hope, and what was his connection to cardiology and St George's Hospital?
James Hope was born near Manchester in 1801. His name was never associated with a disease or syndrome or the naming of a physical sign but his skill was to take a new invention, the stethoscope, and to demonstrate its value in the diagnosis of diseases of the heart. After studying for five years in Edinburgh he undertook further study in London, Paris and Milan beofre being appointed as assistant physician to St George's Hospital at Hyde Park Corner. Over the next 5 years he saw over 20,000 patients that we admitted and a further 15,000 outpatients. He was appointed to the staff of the hospital as physician in 1839 at the age of 38. James Hope’s major contribution to cardiology was to understand the origin of the sounds heard when examining the heart. Laennec, the inventor of the stethoscope, thought that the first heart sound was due to the contraction of the ventricles and the second sound due to contraction of the atria. Hope conducted experiments on the exposed heart of a stunned donkey and correlated the sounds with the movement of the beating heart. He used a dissecting hook to block the aortic valve from closing and found that he was able to eradicate the second heart sound correctly concluding that the second heart sound was due to the closure of the aortic valve. Like many new inventions many doctors were afraid of using the stethoscope. To aid this in July 1838 James Hope hosted a public demonstration on the use of the stethoscope. This was described in the London Medical Gazette: "The following experiment... affords demonstrative proof that the diagnosis in question, usually supposed to require years of experience, may be efficiently taught in the brief space of ten minutes; and I communicate it to you in the hope that, through the medium of your valuable journal, it may by encouraging the diffident proof subservient to the progress of medical science." Sadly James Hope career was cut short by tuberculosis and he died in 1841. He was one of the first physicians interested in cardiology and is remembered for his important contributions to the science of cardiology. His memory lives on for all those staff and patients who come into contact with James Hope ward. Hope J. (1833). A treatise on the diseases of the heart and great vessels: comprising a new view of the physiology of the heart's action according to which the physical signs are explained.  It is the ultimate accolade for an inventor or manufacturer when their name becomes part of the language or is used as a verb to describe a action. Examples include Hoover, Xerox and Google. In cardiology the stent, which is used to treat patients with narrowed coronary arteries shares this unique position as a noun and a verb but where did the word stent come from and why are stents called stents? Mosby's medical dictionary defines a stent as "1. a compound used in making dental impressions and medical molds. 2. a mold or device made of stent, used in anchoring skin grafts and for supporting body parts and cavities during grafting of vessels and tubes of the body during surgical anastomosis." In 1856 Dr Charles Stent invented a material made of natural latex mixed with stearine, talc and red dye which resulted in a stable flexible material which could be used to make dental molds. Some years later the famous plastic surgeon Harold Gillies in his 1920 book Plastic Surgery of the Face, wrote "The dental composition used for this purpose is that put forward by Stent, and a mold composed of it, is known us a "Stent." This is probably the first use of Stent's name as a noun. The use of the word stent to describe a scaffold in the vascular system was by Dr Charles Dotter who in 1983 published his report on "Transluminal expandable nitinol coil stent grafting." The first coronary stent was implanted in 1986 by Jacques Puel in Toulouse and together with Ulrich Sigwart they were been credited with developing the concept of the coronary stent. This device is now used in more than 80% of angioplasty procedures and provides a scaffold for the local delivery of drugs to the artery to prevent re-narrowing at the site of implantation. 
 Syndrome X is the name used by cardiologists to describe patients who have typical symptoms of angina, an abnormal exercise ECG but apparantly normal unobstructed coronary arteries. The cause of the syndrome is much debated and many theories as to its aetiology abound. Most of the research focus has been on the coronary microvessels which are believed to have impaired function with an inability to dilate appropately. Clinically these vessels are difficult to assess since the microcirculation of the heart cannot be easily imaged or measured using standard investigations. Almost 50 years after the first description of Syndrome X still it remains somewhat enigmatic. Even the name suggests an element of mystery reminiscent of the "X files" used to refer unsolved cases in the popular television drama of the same name. So why and who named it Syndrome X in the first place?
By the late 1960's, with the introduction of selective coronary angiography, it was becoming apparent that not all patients with angina had narrowed coronary arteries. Indeed nowerdays we recognise that ~40% of patients having a coronary angiogram will have no signficant obstruction to blood flow. In 1967 Likoff published a paper in the New England Journal of Medicine reporting "The Paradox of Normal Selective Coronary Arteriograms in Patients Considered to Have Unmistakable Coronary Heart Disease". This paper described 15 pre-menopausal women with smooth coronary arteries but typical cardiac sounding chest pain and an abnormal ECG during bicycle exercise. Once the observation was made further research was performed to try and understand the mechanisms involved. In 1973 Arbogast and Bourassa published a paper examining heart function during atrial pacing in patients with angina and normal coronary angiograms. These patients were referred to as "group X" and they were compared to people with narrowed coronary arteries who were referred to as "group C". These authors showed that rapid pacing of the heart resulted in reduction in cardiac function in patients with coronary disease but paradoxically an enhancement the patients in group X. This observation provoked much debate then and is still difficult to understand because abnormalities of heart function usually go hand-in-hand with reductions in coronary blood flow. The observations with "group X" led to the label of syndrome X being used in the accompanying editoral by Harvey Kemp to describe these patients. This spread though the medical literature and now there are over 1200 papers and articles published on cardiac syndrome X. Likoff W, Segal BL, Kasparian H. Paradox of normal selective coronary arteriograms in patients considered to have unmistakable coronary heart disease.N Engl J Med. 1967 May 11;276(19):1063-6 Arbogast R, Bourassa MG. Myocardial function during atrial pacing in patients with angina pectoris and normal coronary arteriograms. Comparison with patients having significant coronary artery disease.Am J Cardiol. 1973 Sep 7;32(3):257-63. Kemp HG Jr. Syndrome X revisited. J Am Coll Cardiol. 1991 Feb;17(2):507-8. 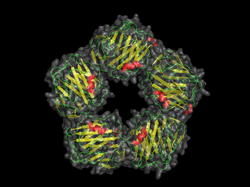 Topological structure of C-reactive protein C reactive protein (CRP) is one of the most widely performed blood tests in patients admitted to hospital. Alongside a full blood count, kidney and liver function test CRP levels give an indication of possible bacterial infection or inflammation. Sometimes, especially in the elderly, it may be the only laboratory test indicating a patient is seriously ill. When discussing CRP on ward rounds one question I commonly ask is: "So what does the "C" in CRP stand for?" Most medical staff will have ordered and interpreted this test dozens of time but they won't have thought about this question. Often answers such as "complement" or even "cardiac" are suggested but neither is correct. The discovery of CRP dates back to 1930 when William Tillett and Thomas Francis, working at the Rockefeller Institute, published a paper in the Journal of Experimental Medicine entitled: "Serological reaction in pneumonia with a non-protein somatic fraction of the pneumococcus." They were investigating the Pneumococcus, a bacteria responsible for pneumonia, meningitis and other serious infections. The pneumococcus was known to contain two distinct constituents. One was present in the bacterial capsule and the other a nucleoprotein in the cell body. Tillett and Francis identified a third chemically distinct, non-protein somatic fraction which was heat and acid soluble. They designated this "Fraction C". Their key discovery was that if sera from patients with bacterial infections was mixed with the C-fraction of the pneumococcus an immediate precipitation was observed. 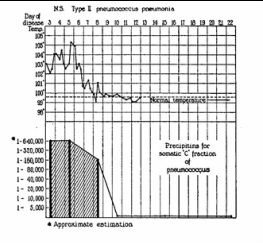 Time course of CRP reaction as patient recovers They went on to show that the precipitation still occured when a patients serum was highly diluted and that reaction appeared promptly following the onset of the illness and disappeared quickly in the recovery phase. In their first paper they called this C-reactive substance but in later showed it to be a protein and renamed C-reaction protein.
CRP is widely used today and is useful for assessing patients with suspected infections. In cardiology CRP is valuable in monitoring the response to antibiotic treatment in patients with infective endocarditis. It is also increased in patients with acute coronary syndromes predicting risk of death, cardiac rupture and recurrent myocardial infarction. More recent evidence has also emerged that CRP might have a role in predicting people at increased risk of heart disease. The precise biological role of CRP is still debated and it is unclear 80 years after its discovery whether it is a marker of disease or an immune mediator but whatever its role it is certainly a very valuable biomarker in everyday clinical practice. Tillett WS, Francis T. Serological reactions in pneumonia with a non-protein somatic fraction of pneumococcus. J Exp Med. 1930 Sep 30;52(4):561-71. |

Dr Richard BogleThe opinions expressed in this blog are strictly those of the author and should not be construed as the opinion or policy of my employers nor recommendations for your care or anyone else's. Always seek professional guidance instead. Archives
August 2023
Categories
All

|
 RSS Feed
RSS Feed