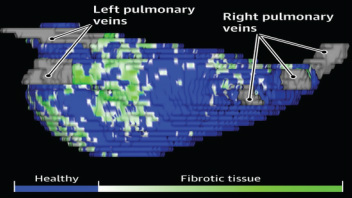
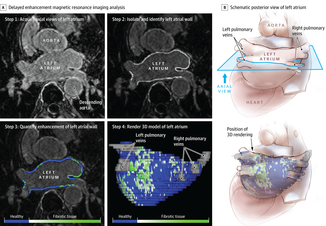
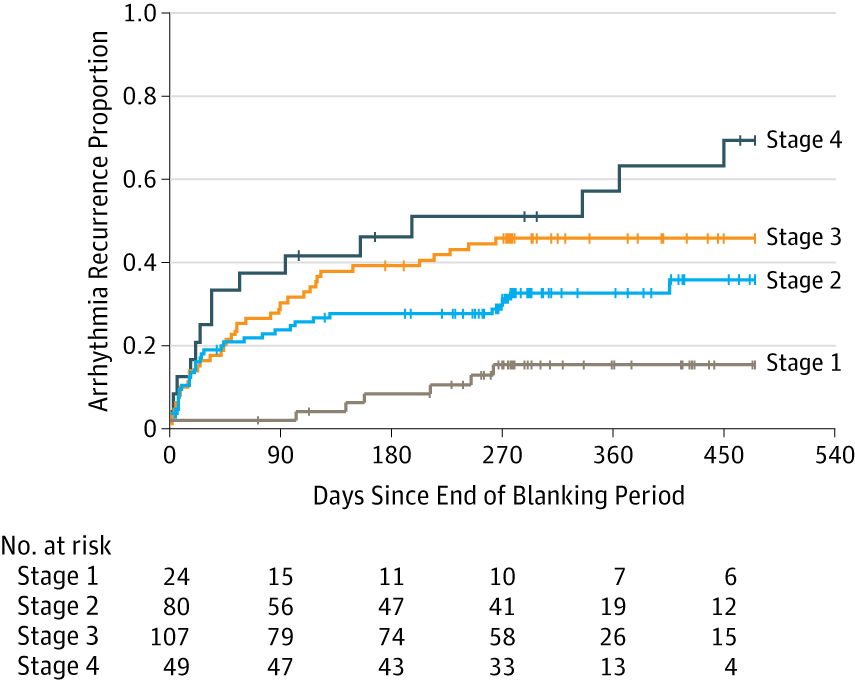
 The success of ablation for atrial fibrillation (AF) is variable. It depends on the patient, it depends on the doctor. Traditional thinking was that people with a structurally normal heart on echo who had paroxysmal AF would do well with ablation. Those people with dilated left atrium and long standing persistent AF would not do so well. But how good are we really at selecting who will benefit from ablation? Pulmonary vein isolation (PVI) also known as AF ablation is the commonest catheter based procedure for the treatment of AF. The aim is to electrically isolate the pulmonary veins from the atrium because it is believed that ectopic beats arising in these veins are responsible for triggering episodes of AF. Despite the enthusiasm of some cardiologists for this procedure and the very large number of ablation procedures carried out daily around the world the long term results of randomised clinical trials are mixed to say the least with many patients relapsing back into AF within a year or requiring multiple procedures. Despite the best efforts of cardiologists the current clinical parameters we assess fail to define properly which patients will have successful maintenance of sinus rhythm after an AF ablation. Recent work performed at the University of Utah however is allowing us to think about the selection question differently. For a long time we have known that fibrosis in the atrium is important. The difficulty is how to measure fibrosis in people non-invasively. The Utah group have developed a method for assessing the amount of fibrosis in the left atrium using MR scanning. Using this information they are then able to show that the amount of fibrosis predicts which patients will respond well to ablation and remain free of AF and which patients will have a recurrence. The DECAAF study recently published in JAMA looked at 329 patients about two thirds of whom had paroxysmal AF and the rest persistent. They performed a special sequenced MR scan on all the patients. In 83% it was possible to obtained a scan of good enough quality to interpret. These patients then had an AF ablation were followed up for at least a year. At the end of the study about a quarter of patients were still on Class I or III (i.e. potent) anti-arhhythmic drugs indicating that ablation even if successful is does not mean no need for medication. Also about 5% of patients had a serious complication from the procedure. The MRI technique measured the amount of left atrial fibrosis and this was strongly associated with AF recurrence after removal of confounding variables such as age, hypertension history etc. When the patients were looked at 325 days after the ablation those with stage 1 (<10% fibrosis) had an AF recurrence rate of 15.3%, those with stage 2 (10-20% fibrosis) had a recurrence rate of 32.6%. By stage 3 (20-30% fibrosis) 45.9% were back in AF and stage 4 (>30% fibrosis) 51.1% were in AF. By 475 day the recurrence rate for stage 1 was 15.3% still but the stage 4 patients had increased to 69.4%. The AF phenotype of the patients - paroxysmal versus persistent, young versus old, short versus long history of AF does not predict fibrosis and so a young patient with paroxysmal AF may have extensive fibrosis and therefore a very high risk of arrhythmia recurrence whereas another patient, older and with persistent AF may have little fibrosis and therefore have a very good chance of long term success with AF ablation. The only clinical parameter associated with fibrosis was hypertension. These results suggest that imaging of patients with AF before recommending interventions might improve the management. Allowing us to avoid procedure that are unlikely to benefit patients and to offer them to those with much to gain. I predict that we will see a rise in imaging and tissue characterisation of AF patients over the next few years.
0 Comments
|

Dr Richard BogleThe opinions expressed in this blog are strictly those of the author and should not be construed as the opinion or policy of my employers nor recommendations for your care or anyone else's. Always seek professional guidance instead. Archives
August 2023
Categories
All

|
 RSS Feed
RSS Feed