 In Eric Topol's book The Creative Destruction of Medicine he speaks about how the precipitous convergence of a maturing Internet, increasing bandwith, near ubiquitous connectivity and miniature pocket computers (smartphones) are taking physicians and patients where no one has gone before. Palpitations are a common symptoms in patients attending my clinic. Assessment tries to establish when the symptoms started, how frequently they occurs, how long each episode is, whether there are provoking or relieving factors and whether there are any associated symptoms. I try to see whether the patient thought the rhythm disturbance was regular or irregular. Many times people are vague about the precise nature of the symptoms because it is very subjective and truly difficult to describe. For most patients the frequency of attacks is perhaps once or twice a week at most. What they need is an ECG recorded at the exact time they have symptoms. We still use the so called "24h Tape". in fact these can record for 7 days and don't contain any tape. We use cardiac event monitors such as the Novacor R-test which record loops of ECG for a week or more. One problem with all these devices is that they require wet gel electrodes to be stuck to the skin for long periods which often results in skin irritation and discomfort. The other problem is the so called vanishing arrhythmia that never comes when the monitor is attached. So is there another way to record the ECG which might be useful for someone with intermittent palpitations using a machine which people have to hand most of the time. This is where the AliveCor smartphone attachment comes in. I ordered one recently. It looks and behaves like a protective smartphone cover. Having already downloaded the AliveCor app I was ready to record my single lead ECG within a moment. The quality is remarkable and the device so simple to use. With two dry electrodes on the back of the phone, one for the left and the other for the right hand you can get a lead 1 type ECG. If you want a better P wave (ie lead II or III) why not put the device on the left leg and the right hand which also works superbly. No skin preparation is needed. One of the recordings I made is shown below - you can judge the quality for yourself. This is a typical recording and because it is on a smartphone it is possible to email the file or store it as a PDF. I guess the main limitation at present is the need to possess a smartphone and also the cost of the device which currently retails at £169. Certainly for patients with paroxysmal atrial fibrillation or episodic palpitations this device might be very useful. I am looking forward to using it. For further information about the device and how it works see the dedicate page on my website. 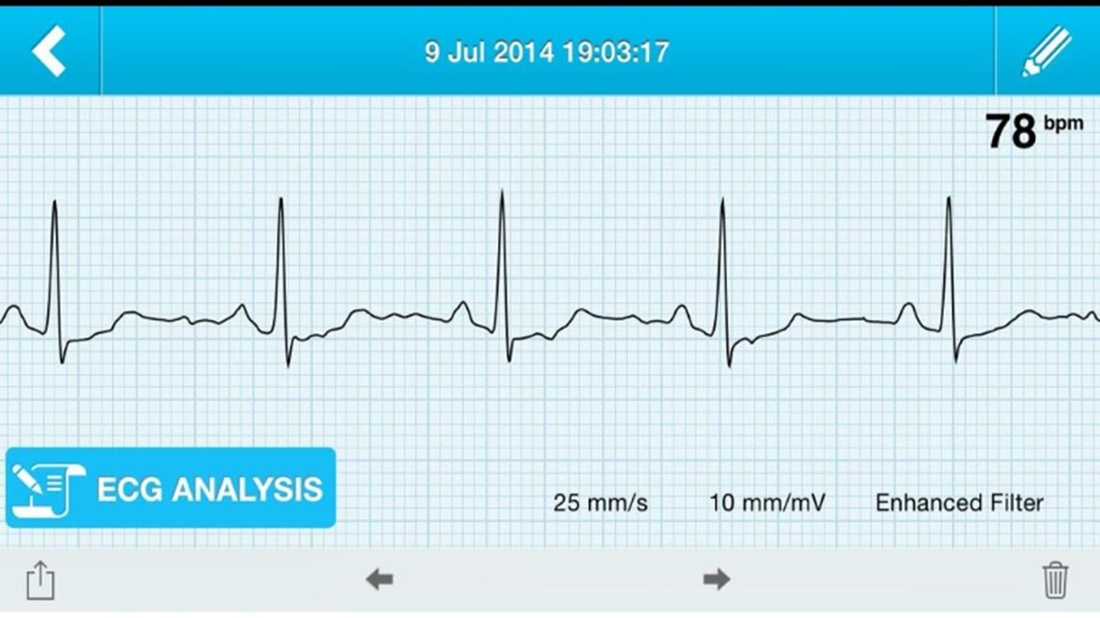
0 Comments
Sometimes I wonder how cardiology practice will changed in the next 20 years. Looking back to how we assessed people with suspected coronary artery disease little has changed in the last two decades. In 1994 we would make an approach with clinical history, examination and then use of the exercise ECG and performing invasive coronary angiography. Developments in imaging have spiralled with echo, MRI and CT all having a more and more domain role in patient assessment. What I believe will change cardiology in the next 20 years is the further development of cardiac CT as a method of not only showing the anatomy of the coronary arteries but going further and assessing the functional significance of any narrowing and the presence of high risk disease. Currently the 64 and 128 slice CT is is good at demonstrating normal coronary arteries in younger people but the technique is not so good in older people when the coronary arteries are calcified or when moderate disease is detected. In these situations cardiologist usually resort to invasive angiography. CT research is driving forward the technique to make assessments of plaque morphology and plaque specific functional data. Current interest is in the measure of ESS which is the the tangential force generated by the friction of flowing blood on the endothelial surface of the arterial wall. In coronary segments with low and disturbed or turbulent flow (low ESS) endothelial cells express proatherogenic genes and development of high-risk lesions. In contrast straight arterial segments with undisturbed laminar flow (normal ESS) has endothelial cells express atheroprotective genes resulting in stable and quiescence plaques. Putting this together it seems that ESS might be a CT measure which can help the cardiologist decide if the patient is at increased risk of heart attack. CT is highly sensitive to identify atherosclerotic plaques this information could be assessed to other risk factor information to identify patients with subclinical CAD and vulnerable plaques. Combining the complex information obtained from CT would realize a more personalized approach to cardiovascular disease prevention and care for each patient. 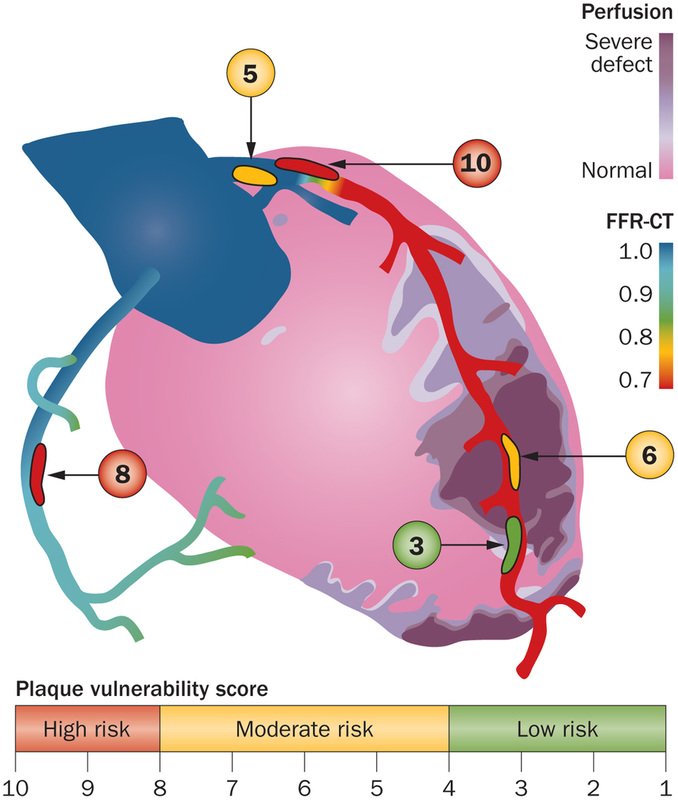 |

Dr Richard BogleThe opinions expressed in this blog are strictly those of the author and should not be construed as the opinion or policy of my employers nor recommendations for your care or anyone else's. Always seek professional guidance instead. Archives
August 2023
Categories
All

|
 RSS Feed
RSS Feed