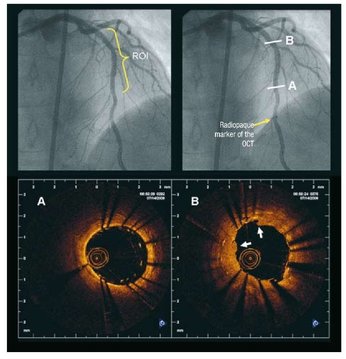
 Angiography of the LAD artery & optical coherence tomography Angiography of the LAD artery & optical coherence tomography The universal approach for deployment of a coronary stents is to use high pressure inflations. This is because high-pressure improves stent expansion and apposition and markedly decreases the incidence of acute and subacute stent thrombosis.
In contrast there is no standard protocol for the duration of the high-pressure inflation. Often when a stent is placed the inflation pressure tends to gradually decrease over time suggesting that there is on going slow stent expansion. If the stent further expands with the same inflation pressure then a rapid inflation/deflation sequence may not adequately expand the stent even if the final angiogram looks good. It is possible that sustained inflation until pressure stabilizes would result in more optimal stent deployment. The possibility of incomplete strut apposition may also be heightened if inadequate time is allowed for stent expansion. A recent study has looked at 12 patients having single vessel stent interventions using the new technique of optical coherence tomography. This is an ultrasensitive method that can visualise the apposition of individual stent struts. After pre-dilation the lesions were stented with no angiographic residual stenosis after high-pressure stent balloon inflation of relatively short duration (“rapid” inflation) with an average inflation time of 28±17 sec. Following an OCT measurement prolonged inflation was performed. The inflation time was chosen such that the pressure in the inflation device was completely stable for at least 30 seconds. In order to achieve this it required much longer periods of inflation for 206 ± 115 sec. The patients appeared to be stable during this long inflation but what is interesting is that the minimal stent diameter and minimal stent area both increased after prolonged inflation compared with rapid inflation. Stent diameter increased by 9% from 2.75 ± 0.44 to 3.0 ± 0.5 (P < 0.0001) and stent area by 18% from 6.63 ± 1.85 to 7.83 ± 2.45. Not only this but stent strut mal-apposition was halved. This is a small study but important as it makes us think once again that the coronary angiographic results is a relatively crude guide to the apposition of the struts and the overall deployment of a stent. We should consider using both high pressure and longer inflations.
0 Comments
Your comment will be posted after it is approved.
Leave a Reply. |

Dr Richard BogleThe opinions expressed in this blog are strictly those of the author and should not be construed as the opinion or policy of my employers nor recommendations for your care or anyone else's. Always seek professional guidance instead. Archives
August 2023
Categories
All

|
 RSS Feed
RSS Feed