 It seemed so simple. If there is a coronary artery narrowing then dilate it with a balloon and insert a stent. The narrowing goes away and the patient is improved. If the artery is the proximal LAD and the narrowing is 90% then surely this must be of benefit, after all, isn't a 90% proximal LAD lesion know as a widow-maker lesion?
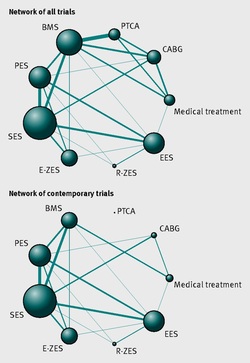
The problem is that despite the intuitive simplicity of this approach cardiologists have struggled to find the evidence to prove that angioplasty does anything beyond reduce symptoms in stable angina. Only last week a commentary in JAMA Internal Medicine called for better patient information about stenting procedures arguing that many patients consented to these procedures thinking they would not only improve their angina but also reduce risk of death and heart attack. Most recent discussions regarding angioplasty have been reached on the basis of the COURAGE trial. When the COURAGE trial is critiqued you often hear that interventional practice is different and if the trial were done using modern stents then the outcomes would almost certainly be different. These comments are often made by cardiologists keen on promoting angioplasty. However the point is critical since there are major differences between the bare metal stents used in COURAGE and the second generation drug eluting stents used today. No one would argue that the current stents are not vastly superior to bare metal and first generation stents in terms of rates of restenosis and acute stent thrombosis. Earlier this week the BMJ published an important meta-analysis of trials of revascularisation in stable angina. Credit should go to the authors for pulling together and analysing the results of a 100 clinical trials and reviewing the information shown in the Web accessible supplement shows how much work goes into pulling these reviews together. The results are fascinating and at provide evidence to support the argument that judging contemporary practice using historical trials may be misleading. The results showed that when comparing coronary artery bypass grafting (CABG) to medication there was a 20% reduction in death. Angioplasty but importantly only with new generation (everolimus or zotarolimus) stents reduced deaths by 25-35%. All other interventional procedures had no effect. CABG reduced myocardial infarction by 21% compared to medical treatment and all angioplasty procedures except bare metal stents and paclitaxel eluting stents also showed evidence for possible reduction. Compared with medical treatment, revascularisation with CABG reduce subsequent revascularisation by 84% and stents reduced revascularisation by 66-73% depending on the type of stent used. So for t the moment it reasonable to conclude that in stable coronary disease CABG reduces the risk of death, MI and the need for revascularisation compared with medical treatment. Stent procedures reduce the need for revascularisation but also improve survival when new generation drug eluting stents are used. So at last there is a glimmer of hope that coronary stents do more than just treat angina in stable coronary disease. This will be music to the ears of many interventional cardiologists but whether this glimmer of hope will turn into a bright beacon or a fizzle out will be largely dependent on the results of the ISCHAEMIA trial.
2 Comments
X
30/6/2014 08:45:06 am
Freedom. 7/7/2014 08:55:12 am
Network meta-analyses are a mixed blessing. Experts argue that by using a bayesian random effects Poisson regression model, you can preserve randomised treatment comparisons within trials. But that begs the question of how you can achieve dependable comparisons between trials, robust enough to guide clinical practice. Unfortunately I was born with loss of function variants on my STATS-WONK alleles and cannot work that out. This network meta-analysis would have us believe that the era of COURAGE has come to an end: thanks to better drug eluting stents and techniques for coronary artery bypass surgery, people with stable coronary artery disease will now experience fewer deaths and myocardial infarctions if they have early invasive treatment. But I couldn’t dig out the figures that would allow me to share any decisions confidently with actual patients. I fear that this meta-analysis, which is very hard to confirm or contest, will simply be used as a pretext for interventionists to return en masse to their bad old habits. Your comment will be posted after it is approved.
Leave a Reply. |

Dr Richard BogleThe opinions expressed in this blog are strictly those of the author and should not be construed as the opinion or policy of my employers nor recommendations for your care or anyone else's. Always seek professional guidance instead. Archives
August 2023
Categories
All

|
 RSS Feed
RSS Feed