 In people admitted to the hospital with cardiac chest pain a subgroup is recognized on the basis of a characteristic ECG change that predicts a high risk of impending extensive anterior myocardial infarction. The ECG has a highly characteristic ST-T segment change in the chest leads and at angiography patients usually have a critical stenosis in the proximal left anterior descending coronary artery.
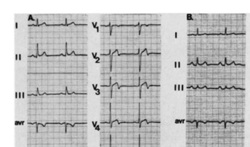
In the original paper published in 1982 in the American Journal of Cardiology they found 26 patients out of 145 consecutive admission had this typical pattern. The description was of abnormal ST-T segments in leads V2 and V3 consisting of an isoelectric or minimally elevated (1 mm) take-off of the ST segment from the QRS complex, a concave or straight ST segment passing into a negative T wave at an angle of 60 to 90 degrees, and a symmetrically inverted T wave. Twenty-five of the 26 patients also had a typical pattern in lead V1: an isoelectric or minimally elevated (1 mm) take-off of the ST segment and a concave or straight ST segment passing into the first part of the T wave at an angle of approximately 135 degrees, followed by T wave inversion. In addition, 22 had an ST-T segment pattern in lead Vl, and sometimes V2 and V3, consisting of a take-off of the ST segment from the QRS complex below the isoelectric line and a convex ST segment passing into a negative T wave at an angle of about 120 degrees with a deep symmetrically inverted T wave. As with many things a picture says a thousand words and the figure illustrated above shows the two patterns. The original paper published in 1982 shows the natural history of this condition if managed conservatively with beta blockers and GTN. They had 145 patients consecutively admitted with chest pain of which 18% had the characteristic ECG pattern and 75% of them who were not operated on developed an extensive anterior wall infarction within a few weeks after admission. The authors recommended that patients with this ECG pattern should have urgent coronary angiography and revascularization. Cardiologists now refer to this ECG pattern as a Wellens ECG or Wellens syndrome. In a patient with symptoms of chest pain it should prompt the patient to be admitted to hospital irrespective of the troponin level and urgent coronary angiography arranged. This is certainly a situation where coronary revascularisation will reduce the risk of myocardial infarction.
0 Comments
Your comment will be posted after it is approved.
Leave a Reply. |

Dr Richard BogleThe opinions expressed in this blog are strictly those of the author and should not be construed as the opinion or policy of my employers nor recommendations for your care or anyone else's. Always seek professional guidance instead. Archives
August 2023
Categories
All

|
 RSS Feed
RSS Feed