|
Which one would you choose? The healthy option or the chocolate bar? Perhaps your head says apple but your stomach says chocolate. If I told you the apple has 59 kilocalories and the Twix has 246, 18% of you would choose the apple. If I told you the apple has 247 kilojoules and the Twix has 1,029, 41% of you would choose the apple.
When people are faced with healthy versus unhealthy choices the way in which nutritional information is presented influences that choice. If you test this in people with a low prior interest in energy information the probability of choosing the apple increases from 3% to 59%.
We are exposed to this type of unit effect all the time. When we buy something for £9.99 we focus on the £9. When you are told a product costs just £1 a day rather than £30 a month and when a waiting time for treatment is 18 weeks rather than 4 and a half months. The way we present information has a significant effect on the choices people make so we should consider that when giving health promotion advice. How to Make a 29% Increase Look Bigger: The Unit Effect in Option Comparisons
0 Comments
 Stop smoking, lose weight, and change your diet! As doctors we are constantly giving advice to people how to improve their health. We think these messages are clear. You are overweight, your blood pressure is too high and obesity increases blood pressure so lose weight. But much of this advice goes unheeded. How can we make it more effective. One way is to use the concept of appealing to Social Norms. We've all seen those signs in hotel bathrooms asking us to reuse the towels. Its good for the environment and after all you don't change your towel everyday at home? But only about a third of people actually reuse the towels. How can we increase that and does the way the message is conveyed alter the likelihood the towels are reused? A study published in the Journal of Consumer Research looked at this question and the results are interesting.
They had 2 messages for the hotel guests. A standard one focused on environmental protection "HELP SAVE THE ENVIRONMENT. You can show your respect for nature and help save the environment by reusing your towels during your stay." The other message had a descriptive norm informing people that a majority of other guests reused their towels: “JOIN YOUR FELLOW GUESTS IN HELPING TO SAVE THE ENVIRONMENT. Almost 75% of guests who are asked to participate in our new resource savings program do help by using their towels more than once. You can join your fellow guests in this program to help save the environment by reusing your towels during your stay." The messages were randomly assigned to different hotel rooms. Towel reuse went up from about 30% in the standard message to 44% with the descriptive norm message. With further adjustment to the wording “JOIN YOUR FELLOW GUESTS IN HELPING TO SAVE THE ENVIRONMENT. In a study conducted in Fall 2003, 75% of the guests who stayed in this room participated in our new resource savings program by using their towels more than once. You can join your fellow guests in this program to help save the environment by reusing your towels during your stay", they increase towel reuse to 50%. Descriptive norms improve towel reuse at least in hotel bathrooms but does this work in other areas. The Behavioural Insights Team, the so called Nudge Unit of the Cabinet Office, looked at charitable donations in wills. The average donation was £3,300. When people rang to book a will-writing appointment they were randomly assigned to one of two groups of will-writers. The first took their details and then asked "Would you like to leave any money to charity in your will?". The second said "many of our customers like to leave money to charity in their will. Are there any causes you’re passionate about?” The first or "Plain Ask" method had no effect on donations but the second social normative doubled the average donation to £6,661. The results are important for hoteliers and charities but also have implications for doctors and nurses trying to improve the uptake of health promotion programs. If we can introduce social norms into our recommendations this is likely to improve the chance that our advice is followed.  Assessment of patients with CT scans of the heart is becoming more common. A CT scan can detect the earliest signs of coronary artery disease which manifest itself as calcification and remodelling of the arteries before any stenosis or symptom develops and way before it can be detected by exercise treadmill or other functional tests.
When patients are found to have moderate coronary artery disease or coronary calcification detected on a CT they are offered treatment with intensive risk factor modification with aspirin, statins and ACE inhibitors. Usually they ask two questions. First will these treatments reverse the coronary artery disease and second how can they monitor the situation going forward to find out if the treatment is working beyond simple measures like the absence of symptoms or change in cholesterol levels. Traditionally repeating the CT scan after a time interval has not been recommended however a recent paper from the MESA study group has questioned this. They looked at the value of repeat cardiac CT scanning to detect changes in coronary artery calcification (CAC) and to see if this was associated with increased risk of cardiac events such as heart attack. They studied 5,682 people with a baseline and follow-up CAC 2.5 years later. The results showed an annual increase in CAC score of about 25. In people with a CAC of 0 at baseline a 5-unit annual increase was associated with a 1.5 fold increase in risk of heart attack. In those people with a raised calcium score at baseline, for every 100 annual increase there was a 1.3 fold increase in risk. In those people with an annual progression of more than 300 there was a 6.3 fold increase in risk. So progression of CAC is associated with an increase risk of adverse outcomes for patients and monitoring progression of disease with a CT scan after an interval of about 2.5 years is a reasonable strategy. If progression is <100 then the patient can be reassured that their treatment is working and there risk is not increasing. If there is progression of >300 then they might benefit from a more intense treatment program.  When patients come to a hospital outpatient clinic it is common for them to be asked about the medication they are taking. As a physician, medicines are your main weapon against disease and even as an interventional cardiologist I spend most of my time intervening with my pen rather than with catheters. It is essential for the doctor to know which medication the patient is taking and in what dose. Some patient with angina, high blood pressure or diabetes are prescribed over 10 different medications, but how many of them are being taken?
Compliance is understood to mean acting in accordance with advice of the prescriber. The word is linked with an old-fashioned paternalistic attitudes towards the patient by the prescriber and so instead the idea of concordance, implying that prescriber and patient were in general agreement about the drug regimen is preferred. Some people prefer the term adherence which implies a steady observance or maintenance. So in the clinic how do we really know whether our patients are adhering to their medications as prescribed? A study just published in Heart looked at this question in 208 patients referred their secondary care hypertension clinic. Using an HPLC assay to detect 40 of the most commonly prescribed antihypertensive medications they ran samples of the patient's urine to see if the drugs on prescription chart were present in the urine. Shockingly in 25% of patients only some of the blood pressure medications were found and in 10% none were found. This follows on from a study in Germany that looked at 108 patients with resistant hypertension. Of these 15 patients had secondary causes of hypertension and 17 achieved blood pressure control by the addition another drug. In the remaining 76 patients, using the same type of HPLC analysis of the urine, 53% of patients were non-adherent to the prescribed medication and 30% were not taking any blood pressure medication at all. Patients with resistant hypertension are often sent for expensive investigations such as MRIs, blood and urine tests looking for secondary hypertension often with normal results. Apart from higher BP levels and elevated heart rate, adherent and non-adherent patients are indistinguishable which supports the idea that a doctors impression, patient's interviews or pill counts are not reliable markers of adherence. With the results from these studies in mind a formal check of adherence to treatment using a urine analysis would be helpful. Of course this can't give the whole picture since it is also recognised that patients adherence to treatments increases around the time of clinic appointments. In the future it is likely that we will be able to monitor medication adherence. New smart pills containing a silicon chip the size of a grain of sand are already a reality. Composed of trace amounts of magnesium and copper, when swallowed, they react with stomach acid generating a tiny voltage which can be detected by a special skin patch and relayed to a smartphone. These can be built into a medication and would allow doctors to know if medication has been taken and also act as a remind to the patient who might have forgotten to take their tablets. With some medicines such as the new oral anticoagulants addition of this technology could be very cost effective as improved adherence is very likely to improve patient outcomes.  On Sunday about 35,000 people will line up to run the London Marathon. Along the route there will be 1,500 St John first aiders and 150 doctors, physiotherapists and podiatrists. The majority of runner's medical problems involve blisters and muscle cramps however what always makes a headline is if a runner dies or has a cardiac arrest during the marathon.
Fortunately cardiac death during a marathon occurs very rarely (1 in 80,000 runners). Since 1981, when the London Marathon started, there have been eight cardiac deaths. Five of them were from coronary heart disease, two from hypertrophic cardiomyopathy and one from arrhythmogenic right ventricular cardiomyopathy. So far all the cardiac deaths have been in men. As the race day gets closer some runners seek advice as they are concerned about the risk of having a cardiac problem during the marathon. So how should a prospective marathon runner be assessed? I divide runners into two groups. In men aged more than 40 years the main cause of cardiac problems in an marathon is due to coronary artery disease. In women and younger men it is usually due to undiagnosed structural heart disease, usually hypertrophic cardiomyopathy. Assessment involves taking a detailed clinical history looking for symptoms of chest pain, shortness of breath, dizziness or blackouts associated with exercise. We document any cardiovascular risk factors and family history of sudden cardiac death or cardiac diseases. A cardiovascular examination is performed looking for murmurs, measurement of blood pressure and pulses. The cardiologist will usually do an electrocardiogram and often an echocardiogram to rule out structural heart disease In men over 40 or those with risk factors for ischaemic heart disease an exercise treadmill test is helpful to look for any evidence of coronary artery disease. Running a marathon is a gruelling event which places huge stresses on the heart and musculoskeletal systems but fortunately the risk of a cardiac problems is very low and the majority of patients will compete the marathon without problem.  When discussing revascularisation procedures (coronary artery bypass grafting (CABG) or stents), patients often ask: How long will my bypass/stent last? There is no easy answer to this question. I have patients with stents implanted 20 years ago which are still working perfectly and also known people who had a CABG in the 1980’s where all the grafts are in excellent condition. Conversely patients may return rapidly after surgery with graft failure or develop critical in-stent restenosis within months of angioplasty.
Results from randomised clinical trials of stents versus surgery such as the SOS and SYNTAX favour CABG as superior treatment compared to stenting. CABG appears to be associated with a lower likelihood of repeat revascularisation. But there is a problem with these trials. Inherent clinician bias usually favours repeating angiograms in patients treated with stents who develop symptoms after the procedure compared to those patients who have received treatment with CABG. Since the clinician and the patients are not blinded to the original treatment this belief that surgery is a more robust and reliable method of revascularisation is likely to increases the rate of repeat angiography which leads to a high rate of repeat revascularisation. So what is the rate of CABG vein graft occlusion? A recent paper looked at this question in 1829 patients who had a coronary angiogram within 12-18 months after CABG and were then followed for a further 3 years. Within 18 months after CABG 43% of patients (770/1829) had at least one vein graft occlusion. The identification of this occlusion was associated with a 5-fold increase in repeat revascularisations procedures although it did not lead to a higher number of heart attacks or deaths compared to patients whose grafts were all patent. There rate of revascularization procedures within 14 days of angiography demonstrating a vein graft occlusion shows the power of the occlulostenotic reflex as discussed before in an earlier blog. Since the angiography was protocol, and not symptom, driven the identification of the stenosis on an angiogram was enough to result in a repeat revascularisation procedure with a stent. What is the reason for the graft occlusion? Surgical technique, quality of the vein graft and target vessels or is it perhaps that the stenosis didn’t need bypassing in the first place. The FAME study using pressure wire showed that 20% of coronary arteries with significant stenosis (70-90%) on an angiogram were not associated with ischemia and in such cases vein graft failure could easily ay occur without clinical consequence or symptoms. So when answering the question about the longevity of a bypass graft we should say that nearly half of patients will lose at least one graft within 18 months of surgery but the chance that it will cause harm to the patient is low unless someone discovers that it is occluded.  Bergamot a member of the citrus family which is found in the Calabria region of southern Italy. The fruit is a source of essential oils which when added to Earl Grey tea result in the unique scented flavour of this drink. Yesterday national newspapers articles appeared suggesting that Earl Grey tea was as "effective as statins in the fight against heart disease." Is this too good to be true?
The newspapers reported a study in rats published in the Journal of Functional Foods. The authors from Italy showed that extract of bergamot fruit reduced cholesterol levels in these animals and that it was as effective as simvastatin. Now if you want to write a story for the newspaper it's only a few steps of logic before you can claim that drinking Earl Grey tea is a possible substitute for a statin. This conclusion goes way beyond the experimental data but some patients I talked to yesterday were clearly ready to give up their statin and try the natural approach. Is there any evidence that bergamot can treat heart disease? Bergamot fruit contains high concentrations of polyphenols. This is usually thought of as a good thing but really we are not sure what these chemicals do. They are in a group called anti-oxidants and since oxidation is bad these chemicals are thought of as good. This is a vast over-simplification of a complex and poorly understood area of biology. The anti-oxidant potential of bergamot is found in other fruits such as pomegranates and blueberries. These are commonly referred to as super-foods in the pages of popular magazines and their beneficial properties are often promoted. There are several human studies reporting potent effects of bergamot extract on cholesterol levels. In one study LDL, or so called bad, cholesterol levels were reduced as much as in people taking 20mg of rosuvastatin. This is very interesting and if reproduced is quite an astounding effect. But wait, what of outcome trials, where is the data that these fruit extracts reduce heart attacks and save lives? Of course this is completely lacking and there will never be any large clinical trials to prove effectiveness in reducing cardiovascular disease. This is because such studies cost millions of pounds and at the end even if it proved effective there is no prospect of a patentable medicine. Doctors usually demand strong evidence before they prescribe drug treatment and this is true in the field of cholesterol lowering drugs or is it? Every year millions of doses of a cholesterol lowering drug called ezetimibe are prescribed for patients intolerant of statins or in whom cholesterol cannot be reduced enough by statins. Ezetimibe definitely lowers cholesterol but is there is scant evidence that it reduces heart attacks or deaths from heart disease. The IMPROVE-IT trial (simvastatin versus a combination of simvastatin/ezetimibe) started years ago and the results are still awaited. Meanwhile doctors continue to prescribe ezetimibe with enthusiasm. Apart from more evidence that it lowers cholesterol there isn’t too much difference between ezetimibe and bergamot fruit extract when it comes to outcome trials. Patients often favour a natural approach but is important to remember that fruit extracts simply contain chemicals and chemicals sometimes have unwanted effects. For example pomegranate juice can interact with drugs like warfarin leading to serious consequences as we previously reported. So where do we go from here? If you enjoy Earl Grey tea continue to enjoy it as a drink but not for its medicinal properties. If you don’t like Earl Grey tea, no problem because there is almost certainly no health benefit in drinking it. If your statin is working, keep taking it. If your statin isn’t working or you are getting unacceptable side effects such as severe muscle aches which have been proven to be due to the statin by a period of withdrawal and re-challenge then you might discuss taking an alternative with your doctor. Whether this involves the recommendation of bergamot extract or ezetimibe is a matter of opinion.  In the Summer of 2012 David Brailsford presided over Team GB’s incredible haul of cycling medals in the Olympic games. What was the secret of this team’s success? The simple answer was there wasn’t one secret but as Dave Brailsford said it was the aggregation of marginal gains. Performing a coronary angioplasty can take as little as 15 minutes but even with the simplest procedure there are many different choices which the operator needs to make and each of these influences the outcome of the procedure and the risk of complications. Close attention to detail, wise choices and the sum of the marginal gains makes the difference between getting a bronze and achieving gold.
Here is an example. The patient is a 75 year old obese man with diabetes and hypertension. He has a stenosis in the mid right coronary artery. The artery is mildly calcified and a somewhat tortuous. Dr Groin is a default femoral operator. With a 6F sheath, a right Judkin’s guide catheter and a hydrophilic guide wire most cases can be done. Groin access takes but a moment and the coronary artery is easily intubated, the wire glides through the vessel with its usual speed and hydrophilic coating. Within moments the lesion is pre-dilated with a balloon. Then comes the stent but there is a problem, the tortuousity and the calcification makes the stent difficult to track through the vessel. The JR4 catheter does not give any support and the stent cannot be manoeuvred into the correct place. A buddy wire is passed but still the stent won’t track to the lesion. Further ballooning is performed in the vessel which results in a small dissection and without the ability to deliver a drug coated stent they try a bare metal stent which is finally deployed with a reasonable result. The procedure takes 75 minutes and there is 300ml contrast used. An angioseal vascular closure device is deployed but does not quite seal the artery completely and the patient develops a haematoma. The patient eventually leaves the hospital 4 days later. His procedure was a success, the vessel was stented but was this as good as it could possibly be. Dr Wrist usually takes the radial approach. A 5Fglideliner sheath and a 6F AL1 guide catheter are used because the vessel is calcified and somewhat tortuous and he thinks that extra support may be needed. The lesion is crossed with a supportive angioplasty wire, the wire is harder to manipulate than the hydrophilic coated wires but once in the distal vessel it gives excellent support and remains very stable. The vessel is tortuous but the AL-1 gives a really good back up support and the lesion is ballooned with a 2.5x12 balloon and then a 3.5x15 drug eluting stent is deployed with a good result. Because the lesion was calcified a further 3.5x12 non-compliant balloon inflation is made to high pressure with a very good angiographic result. The procedure takes 27 minutes and there is 60ml contrast used. A TR band is placed on the wrist with patent haemostasis and the patient is discharged from the hospital 6h later. His procedure was a success, the vessel was stented. Both patients had a successful PCI on paper but Dr Wrist’s procedure was more successful for the patient. The sum of the small parts – access site, catheter choice, wire choice and ability to deliver devices. All of these single decisions feed into the outcome of the procedure for the patient. Alone each one of these things may contribute only a fraction of a percent to a difference in outcome but when they are all put together they can add up and the sum of marginal gains leads to safer and more effective practice. So how do we achieve these marginal gains in practice: Set audacious goals, work with others who share your vision. Focus, Focus, Focus. Collect high quality procedure data, outcomes data and learn from it. Be disciplined to capture every gain.  Earlier this week saw the sudden death of the union boss Bob Crow. The headline from the Evening Standard screamed: "Tube Union boss Dies of Heart Attack." He was just 52 years old.
Despite advances in treatment of acute heart attacks with primary angioplasty many patients still die suddenly within minutes of the onset of chest pain. The problem with coronary disease is that sometimes the first symptom to alert the patient that something's wrong is when a lethal heart attack strikes. Many patients have not experienced symptoms before that to alter them that there might be a problem. Coronary heart disease does not really have any outward physical signs and so detecting people who may have developed the condition but who have no symptoms is difficult. We recognise various risk factors for heart disease such as age, male sex, high blood pressure, diabetes, cigarette smoking, cholesterol and family history but many people have risk factors and do not develop coronary disease. What would be helpful is an outward physical sign, easily detected, which could alter doctors and patients alike that they might not just be at risk of heart disease but more importantly that they might already have diseased arteries. Over 40 years ago in Dr Sanders Frank reported just such a sign which is today has been forgotten by many doctors and is virtually unknown to patients. In a brief letter published in the New England Journal of Medicine Dr Frank reported his observations of a prominent crease in the ear lobe which was usually present in patients he had seen with coronary artery disease. Initially he reported findings in just 20 patients but since then many studies have been completed confirming his findings. One study of over 1000 unselected patients looked at the presence of a diagonal ear lobe crease and coronary artery disease and found a high degree of correlation independent of age. In this study 112 consecutive patients had coronary angiography and an ear lobe creases was the best predictor of narrowed coronary arteries. Other studies followed which confirmed that ear crease was much more common in patients hospitalized after a heart attack compared to age-matched control subjects with no evidence of cardiac disease. These findings have also been repeated more recently using CT scans to detect coronary artery disease. The presence of an ear lobe crease should alert doctors and patients to the possible presence of coronary heart disease. I don't know anything about Bob Crow's medical history but the picture above a close up of his ear with the ear lobe crease clearly visible. So my advice is clear - look at your ears and if your are under 60 years old and see this change mention it to your doctor. 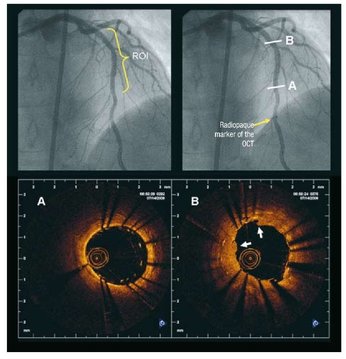 Angiography of the LAD artery & optical coherence tomography Angiography of the LAD artery & optical coherence tomography The universal approach for deployment of a coronary stents is to use high pressure inflations. This is because high-pressure improves stent expansion and apposition and markedly decreases the incidence of acute and subacute stent thrombosis.
In contrast there is no standard protocol for the duration of the high-pressure inflation. Often when a stent is placed the inflation pressure tends to gradually decrease over time suggesting that there is on going slow stent expansion. If the stent further expands with the same inflation pressure then a rapid inflation/deflation sequence may not adequately expand the stent even if the final angiogram looks good. It is possible that sustained inflation until pressure stabilizes would result in more optimal stent deployment. The possibility of incomplete strut apposition may also be heightened if inadequate time is allowed for stent expansion. A recent study has looked at 12 patients having single vessel stent interventions using the new technique of optical coherence tomography. This is an ultrasensitive method that can visualise the apposition of individual stent struts. After pre-dilation the lesions were stented with no angiographic residual stenosis after high-pressure stent balloon inflation of relatively short duration (“rapid” inflation) with an average inflation time of 28±17 sec. Following an OCT measurement prolonged inflation was performed. The inflation time was chosen such that the pressure in the inflation device was completely stable for at least 30 seconds. In order to achieve this it required much longer periods of inflation for 206 ± 115 sec. The patients appeared to be stable during this long inflation but what is interesting is that the minimal stent diameter and minimal stent area both increased after prolonged inflation compared with rapid inflation. Stent diameter increased by 9% from 2.75 ± 0.44 to 3.0 ± 0.5 (P < 0.0001) and stent area by 18% from 6.63 ± 1.85 to 7.83 ± 2.45. Not only this but stent strut mal-apposition was halved. This is a small study but important as it makes us think once again that the coronary angiographic results is a relatively crude guide to the apposition of the struts and the overall deployment of a stent. We should consider using both high pressure and longer inflations. |

Dr Richard BogleThe opinions expressed in this blog are strictly those of the author and should not be construed as the opinion or policy of my employers nor recommendations for your care or anyone else's. Always seek professional guidance instead. Archives
August 2023
Categories
All

|


 RSS Feed
RSS Feed