 If a primary care physician receives a continuous ECG monitor report indicating the presence of short runs of an irregular, non-P wave associated, atrial rhythm lasting <30 s what should they do? What should the reporting cardiologist call this rhythm? What does it mean for the patient now and into the future?
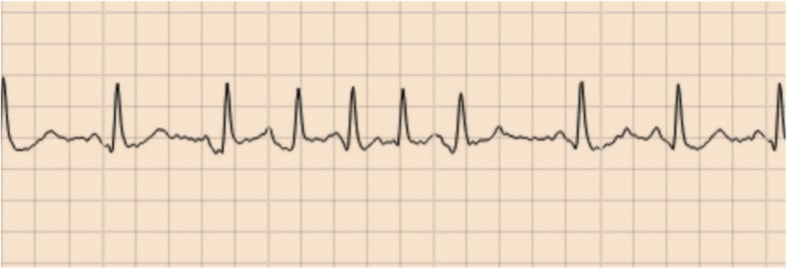
As someone who reports ECG monitors and gives advice to primary care physicians these questions come up a lot. I usually go with the description of the short runs of an irregular ......but just this weekend I came across a new term whilst listening to the This Week in Cardiology podcast - micro atrial fibrillation (micro-AF). This podcast is hosted by the cardiologist Dr John Mandrola and I would say this should be required weekly listening for any practicing cardiologist. It is one of the most well thought through and interesting cardiology podcasts around. John is a "conservative cardiologist" and takes a careful evidence based approach. He's practicing doctor, seeing patients and grapples with the common and difficult clinical scenarios we all come across on a daily basis in our practice. Anyway, back to micro-AF, my new learning of the week. Of course this is not a new phenomenon but something which we all recognize when we are reporting continuous ECG monitors. Diagnosis of AF should be easy. You get an ECG and there 's an irregular rhythm, no P waves and well that is AF but what about when your looking at continuous ECG monitors and there are short runs of irregular rhythm without P waves - how long does this irregular rhythm need to last for it to be called AF. Fortunately there is a definition that it should last more than 30 s for us to consider it AF. Of course this is arbitrary definition - who said 30 s was the right length of time and not 15 or 60 s. Like most of these definitions they emerge from guidelines and a good measure of eminence based medicine. So what about when these irregular, non P-wave containing rhythms which last less than 30 s? What do we call them? I've seen people write things like short runs of atrial ectopics, although an ectopic should be associated with a P wave. I've see short runs of an irregular atrial associated rhythm or short runs of pulmonary vein rhythm. Alternatively we could call them atrial junk (as per John Mandrola) or we perhaps just micro-AF. At face value micro-AF seems like quite an attractive term - after all everyone knows AF and I suppose these are little AF episodes. The term could be useful if they predict AF in the future or are AF but just not 30 s worth of AF then that might be reasonable. What matters is the significance and more importantly what we advise colleagues in primary care and outside of cardiology to do with these patients. I'm concerned if we label them as micro-AF then primary care physicians will be immediately reach for anti-coagulation. If we call them "atrial junk" or other names then we will need to qualify that with some advice, otherwise we are likely to generate significant confusion. So what do these short runs of irregular, non-P wave containing atrial rhythm actually mean. The Swedish group who have coined the term micro-AF have published several studies in this area. They define micro-AF as an irregular tachycardia of sudden onset with episodes of ≥5 consecutive supra-ventricular beats without P waves lasting less than 30 s. In STROKESTOP2 they reported on 3,763 of older people (75 years) screened with intermittent ECG recordings for 30 s 4 times day for 2 weeks. 121 (6%) had micro-AF and of these who then underwent a 2-week period of continuous ECG monitoring AF was detected in 26 (13%). In a control group of 250 people without micro-AF then the continuous monitoring detected 7 cases of AF (3%) So we can conclude that having this micro-AF is associated with a four-fold increase in the risk of detection of AF. In another of their studies called STROKESTOP, 50% of participants diagnosed with micro-AF (this time defined as: abrupt onset, >4 supra-ventricular beats, irregular, no P waves) when followed for 2.4 years ended up with AF detected on monitoring compared with just 10% of patients who did not have micro-AF at baseline. So it certainly looks like having these short runs on the continuous ECG is associated with a higher risk of having longer runs (>30 s) in the future. So what to do if we find AF on continuous monitoring. Is there a case for anti-coagulation of these short episodes of AF? Is it time to anti-coagulate micro-AF. Does any of this reduce the risk of stroke or is it all just atrial junk! We have data on this because the LOOP study reported that in individuals with stroke risk factors an implantable loop recorder (ILR) screening whilst resulting in a 3-times increase in AF detection and anti-coagulation there was no significant reduction in the risk of stroke or systemic arterial embolism. These tell us that screening for AF and then treating it with anti-coagulation is not a worthwhile use of resources and does not benefit the patient. So for now I'm going to avoid the term micro-AF for fear it might cause people to confuse these with AF. Are they atrial junk - well I suppose they could be but I'd feel uncomfortable writing that on a report so for the moment I think the best way is to give a narrative verdict and reassure.
0 Comments
Your comment will be posted after it is approved.
Leave a Reply. |

Dr Richard BogleThe opinions expressed in this blog are strictly those of the author and should not be construed as the opinion or policy of my employers nor recommendations for your care or anyone else's. Always seek professional guidance instead. Archives
August 2023
Categories
All

|
 RSS Feed
RSS Feed