 This is the angiogram of a 48 year old man who exercises regularly and has no cardiac symptoms. His story is not uncommon. He has a medical up every 2 years including an exercise stress test. He completes 9 minutes of exercise without symptoms but there are some ECG changes and cardiology referral is recommended. The cardiologist agrees the exercise ECG is abnormal and requires further investigation. In the absence of symptoms or risk factors for coronary artery disease a CT coronary angiogram was recommended. This surprisingly to the patient indicated a stenosis in the proximal LAD which was then confirmed with an invasive angiogram. Now the cardiologist and patient are faced with a decision: What to do next? There are few things cardiologists agree on but I reckon if you showed 10 interventional cardiologist this angiogram they would all say that something must be done. There might be a discussion about the long term pros and cons of drug eluting stents versus surgical revascularisation but most would agree that medical therapy alone in the absence of revascularisation would represent a sub-standard level of care. Most would agree that a 3.5x23mm drug eluting stent could be placed efficiently with very small risk of complication and an excellent result. There would be complete relief of vessel obstruction and at the same time a reduction in patient and physician anxiety. When it comes to the decision to place a stent are we too strongly influenced by our heart rather than our head. Is it a case of emotion trumping science! The COURAGE study compared optimal medical therapy with stenting in patients with significant coronary disease. After 7 years of follow up in COURAGE study was there was no significant difference between stent treatment and medication. But what of patients with 90% stenosis in the proximal LAD the so called "widow-maker" lesion. Surely patients with this pattern of coronary disease benefit from revascularisation? 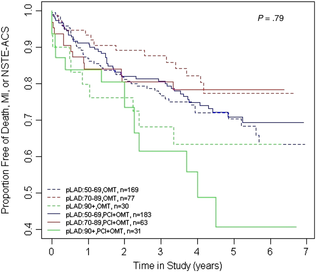 A recent paper from the COURAGE study looked at just this group of patients and found that there was no significant difference between the patient treated with stents or optimal medical therapy. The figure on the left shows the that the group of patients with >90% stenosis in the proximal LAD did not fair well over the 7 years. The surprising thing is that those treated with angioplasty and bare metal stenting (lowest solid green line) appeared if anything to fair less well than those treated with optimal medical therapy (second lowest green dotted line). The presence of proximal LAD disease as a rationale for favouring stenting was therefore not proven. This finding is provocative and instructive.
If you ask interventional cardiologists (and this has been done in focus groups) they will acknowledge that stenting offers no reduction in the risk of death or heart attack in patients with stable coronary artery disease but despite this they generally believe that stenting does benefit such patients. One senior cardiologist said to me that he preferred to treat the cause of coronary artery disease with a stent rather than merely manage the symptoms with tablets. Reasons for performing stenting include belief in the benefits of treating ischaemia, the open artery hypothesis, potential regret for not intervening if a cardiac event could be averted, alleviation of patient anxiety and medico-legal concerns. If asked, most cardiologists believe that the oculo-stenotic reflex prevails and all significant and amenable stenosis should receive intervention even in asymptomatic patients. When cardiologists are challenged about the lack of evidence of adding stenting to optimal medical therapy in preventing future coronary events most still feel that any patient with significant coronary disease should get a stent even whilst acknowledging the evidence. This disconnect between knowledge and behaviour reflects the discordance between cardiologists’ clinical knowledge and their beliefs about the benefits of angioplasty and that non-clinical factors have substantial influence on cardiologists' decision making. So what happened to this patient? I will leave you to decide and to post your thoughts and comments.
3 Comments
Josh Chai
21/2/2014 04:51:48 pm
Great article - admittedly I haven't read the whole AHJ paper but the graph you showed flagged up another interesting observation. No doubt we now know stenting doesn't add additional benefit to OMT in stable CAD but the real separation of the survival+event curve was the initial severity of pLAD lesion. Since lesion severity (usually) doesn't affect stent choice, this effect is likely intrinsic to the lesion itself, hence reflect / support the systemic nature of atherosclerotic diseases. When a severe pLAD lesion is seen angiographically, there are more than likely many more developing plaques in the same or neighbouring vascular territory with lesser severity / with outward eccentric remodelling that are not visible on angiography. This highlighted two important unmet clinical needs: (1) current atherosclerosis is very inadequate and (2) successful future treatment strategy beyond lipid therapy depends on targeting systemic plaque biology rather than massaging individual lesion. To me, the future is very interesting for interventional cardiology:-)
Josh Chai
21/2/2014 11:14:53 pm
Correction:- The first unmet clinical need should read "(1) current atherosclerosis imaging is very inadequate".
Garry Lee
23/6/2014 05:56:51 pm
This kind of thing will always be present in medicine. E.g. Urologists questioned at a large conference as to whether they would choose radiotherapy or surgery for prostate cancer give them equal choice UNTIL they get it themselves in which case they nearly all plump for surgery. Your comment will be posted after it is approved.
Leave a Reply. |

Dr Richard BogleThe opinions expressed in this blog are strictly those of the author and should not be construed as the opinion or policy of my employers nor recommendations for your care or anyone else's. Always seek professional guidance instead. Archives
August 2023
Categories
All

|
 RSS Feed
RSS Feed