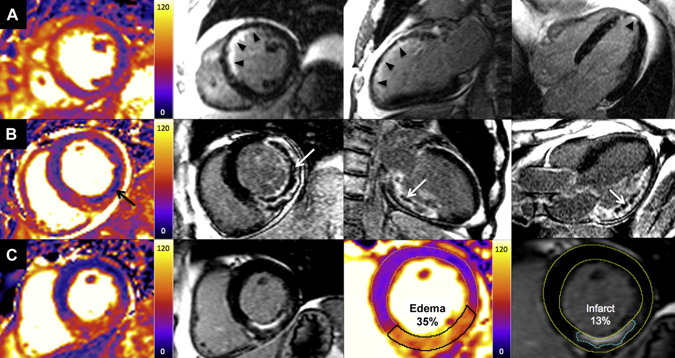
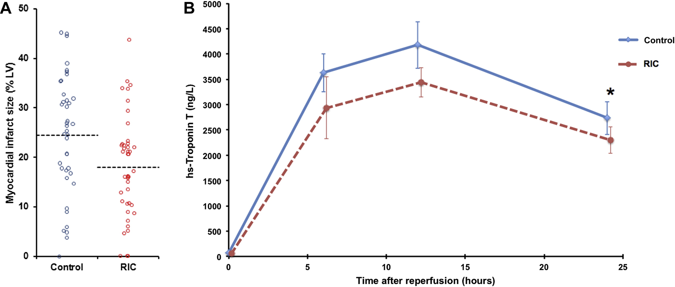
 A bizarre idea? Could squeezing your arm with a blood pressure cuff during primary angioplasty reduce the amount of heart muscle damage. You might be sceptical but this low tech idea is based on some interesting data built up over the last 20 years and it is not as silly as it first might seem. Research published this week in JACC Intervention shows the results of a clinical trial which studied patients admitted to hospital with STEMI type heart attacks. The patients were treated with primary PCI but also had a blood pressure cuff placed on their arm. In half the patients the cuff was inflated to 200mmHg pressure for 5 minutes then released for 5 minutes and this was repeated 3 times, in the other half the cuff was left un-inflated. The idea behind this intervention was to produce a phenomenon known as Remote Ischaemic Post-Conditioning. The trial results showed that cuff inflation reduced the amount of heart muscle damage based on troponin rise and measured by MR scans. The cuff inflation also reduced the amount of oedema or swelling in the heart.
What is the mechanism behind this effect? Trying to reduce the size of heart muscle damage during a heart attack is the primary aim of treatment. Building on the early work of Brunwald in the 1970's the open artery hypothesis was finally realised with the advent of thrombolysis which dissolved the clots in the coronary arteries which caused acute myocardial infarction. Although successful this treatment failed in about 40% of cases and has now been replaced by primary angioplasty. The problem with these treatments is that although they restores the flow of blood to the heart muscle they may also cause reperfusion injury. This is where the injured heart muscle is damaged by free radicals and other toxic substance released when the blood flow is restored.
There has been huge interest in developing drugs which might protect the heart during this reperfusion period but although many have shown promise in the laboratory this has not been translated into benefit when tested in patients. The only treatment to have crossed this translational canyon is one called ischaemic conditioning. Nearly 30 years ago Murry et al. showed that four cycles of 5 minutes of coronary artery occlusion and 5 minute reperfusion protected the heart from a subsequent longer period of sustained occlusion. This effect was called ischaemic pre-conditioning. Although interesting it is difficult to see how it could be applied in clinical practice. Other studies later showed however that ischaemic conditioning could be delivered after the initial period of ischaemia and still be protective. This was called ischaemic post-conditioning and whilst not as potent as pre-conditioning the effect was still important. A breakthrough came in 1993 it was shown that the ischaemic signal for this pre and post-conditioning did not need to be delivered at the site of the subsequent injury to be effective. So for example it was possible to make the arm or leg ischaemic and to protect the heart. This was called remote ischemic conditioning and it was this which led to the clinical trial described above. Like many of these types of trials the numbers of patients and the size of the effect is small. It is more hypothesis generating that a game changer but it does pave the way for larger studies to investigate this effect.
0 Comments
Your comment will be posted after it is approved.
Leave a Reply. |

Dr Richard BogleThe opinions expressed in this blog are strictly those of the author and should not be construed as the opinion or policy of my employers nor recommendations for your care or anyone else's. Always seek professional guidance instead. Archives
August 2023
Categories
All

|
 RSS Feed
RSS Feed