 Topological structure of C-reactive protein C reactive protein (CRP) is one of the most widely performed blood tests in patients admitted to hospital. Alongside a full blood count, kidney and liver function test CRP levels give an indication of possible bacterial infection or inflammation. Sometimes, especially in the elderly, it may be the only laboratory test indicating a patient is seriously ill. When discussing CRP on ward rounds one question I commonly ask is: "So what does the "C" in CRP stand for?" Most medical staff will have ordered and interpreted this test dozens of time but they won't have thought about this question. Often answers such as "complement" or even "cardiac" are suggested but neither is correct. The discovery of CRP dates back to 1930 when William Tillett and Thomas Francis, working at the Rockefeller Institute, published a paper in the Journal of Experimental Medicine entitled: "Serological reaction in pneumonia with a non-protein somatic fraction of the pneumococcus." They were investigating the Pneumococcus, a bacteria responsible for pneumonia, meningitis and other serious infections. The pneumococcus was known to contain two distinct constituents. One was present in the bacterial capsule and the other a nucleoprotein in the cell body. Tillett and Francis identified a third chemically distinct, non-protein somatic fraction which was heat and acid soluble. They designated this "Fraction C". Their key discovery was that if sera from patients with bacterial infections was mixed with the C-fraction of the pneumococcus an immediate precipitation was observed. 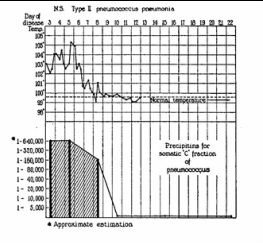 Time course of CRP reaction as patient recovers They went on to show that the precipitation still occured when a patients serum was highly diluted and that reaction appeared promptly following the onset of the illness and disappeared quickly in the recovery phase. In their first paper they called this C-reactive substance but in later showed it to be a protein and renamed C-reaction protein.
CRP is widely used today and is useful for assessing patients with suspected infections. In cardiology CRP is valuable in monitoring the response to antibiotic treatment in patients with infective endocarditis. It is also increased in patients with acute coronary syndromes predicting risk of death, cardiac rupture and recurrent myocardial infarction. More recent evidence has also emerged that CRP might have a role in predicting people at increased risk of heart disease. The precise biological role of CRP is still debated and it is unclear 80 years after its discovery whether it is a marker of disease or an immune mediator but whatever its role it is certainly a very valuable biomarker in everyday clinical practice. Tillett WS, Francis T. Serological reactions in pneumonia with a non-protein somatic fraction of pneumococcus. J Exp Med. 1930 Sep 30;52(4):561-71.
0 Comments
|

Dr Richard BogleThe opinions expressed in this blog are strictly those of the author and should not be construed as the opinion or policy of my employers nor recommendations for your care or anyone else's. Always seek professional guidance instead. Archives
August 2023
Categories
All

|
 RSS Feed
RSS Feed