 This was also published on the British Geriatric Society Blog site
If you watched the news this week you might have thought that the only recommendation in the NICE Atrial Fibrillation Guideline was that doctors should not prescribe aspirin to prevent strokes. In fact most cardiologists and geriatricians stopped using aspirin for this condition several years ago and the NICE recommendation simply reaffirms those issued previously by other professional societies such as the European Society of Cardiology. The real story behind the guidelines was, in my opinion, nothing to do with medication or rate versus rhythm but rather the importance of delivering a personalised package of care for patients with atrial fibrillation (AF). Recognising that AF is a long term health condition there is emphasis on the importance of shared decision making processes particularly around anticoagulation. Alongside the guideline NICE published a Patient Decision Aid to assist with this process. The intention behind this is good but having shown the 36 page decision aid document to several patients today they were overwhelmed by the volume of information they were expected to digest. The aid includes much information that would not be relevant to the individual patient since it tries to cover the risks and benefit of all patients with various stroke and bleeding risks. It uses Cates plots to try and aid the decision making process but each chart has 1000 faces and only looks at the risks/benefits over one year so the faces benefiting from treatment are swamped by hundreds of faces not expecting any benefit. On a practical note NICE assumes that clinicians will have ready access to a colour printer otherwise the red/greens charts look somewhat monotone. The comparison of this decision aid with the highly professional and dynamic way information is presented on the JBS3 risk calculator website is striking and NICE need to up their game to make this and further decision aids much more user friendly. Summarising the information on two sides of A4 is aspirational but possible as has been done with other documents on breast and prostate cancer screening as has been promoted by the work of Gerd Gigerenzer. The guideline emphasises that the patient’s decision regarding anticoagulation will be affected by their own attitude towards risk and NICE say that if patients are provided with the appropriate information about the pros and cons they should be able to decide for themselves about whether to have treatment with anticoagulation or not. This removes the recommendation or opinion of the healthcare provider from the consultation and devolves the decision making to the patient. This represents a change in the doctor patient relationship and the dynamics of the consultation. In my experience, patients want to know the pros and cons of a particular treatment but are also interested in the opinion of the healthcare professional especially if they are well known and trusted. In everyday life we use rules of thumb – so called heuristics and recommendations from friends and family feed into the ability to make complex decisions. Often personal experience and anecdotes are trusted in preference to scientific evidence. To devolve the decision making completely to the patient might be seen as convenient for the healthcare professional. If the patient chooses anticoagulation and then bleeds – it was the patient’s decision to start the treatment, not the doctors. If the patient decides not to take anticoagulation and has a stroke then again it was their decision. In practice clinical medicine is complex and the interaction between a patient and an experienced clinician vital to make a detailed and appropriate assessment. Although stroke and bleeding risk can be calculated using scoring systems these measures are not perfect and derive from large populations which do not necessarily apply to the patient in the consulting room who may have complex multisystem disease and polypharmacy. The risk assessment tools are a starting point of the conversation about treatments. NICE should be commended for placing the patient’s involvement in deciding their management of AF centre stage. This is a clear move in the right direction for patients and should improve both outcomes of this common condition.
0 Comments
In 1958 Mason Sones famously, and apparently accidentally, performed the first coronary angiogram at the Cleveland Clinic. From then on much of the clinical care of patients with ischaemic heart disease was based on research that relied heavily on the visual interpretation of the coronary angiogram. However it wasn't long before papers stared to appear which questioned the accuracy and reproducibility of these visual estimates. One paper from 1976 reported than nearly half the time a group of experienced cardiologists could not agree on the presence of significant coronary artery disease. Other studies followed alleging to to demonstrate the benefits of performing quantitative coronary angiography using computers to assist in the measurement of the degree of narrowing. These methods were more reproducible than eyeballing the angiogram but still there was disagreement and the methodology was time consuming. Take for example this angiogram on shown below. Do you think the this LAD stenosis is flow limiting? Why not vote here and see what others think?
By early 1990's the literature on the accuracy of angiogram went quiet. Cardiologists had other things on their mind - namely coronary angioplasty and stenting. Angiography was the test which fuelled the fire of angioplasty and so the problems with assessment of flow limiting lesions and lesion significance drifted into the background. The occulo-stenostic reflex was strong. Cardiologists needed their angiograms too much to call into question the ability of the test to diagnose and classify the severity of the coronary lesions. This was the era of eminence-based medicine when expert opinion trumped anything else. The poor reproducibility and difficulty in assessment of lesion was forgotten.
When you learn angiography you quickly realise that the interpretation is difficult. When you work for a number of bosses you start to see a difference in their practice. Some always see a moderate lesion as severe, or a severe lesion as critical. The phrase "the angiogram often underestimates the severity of disease" is often be heard in the catheter lab control room as the guide catheter is being opened ready for angioplasty. Whilst there is usually agreement about the mild (<30%) and severe (>80%) lesions it is the moderate ones which are most difficult and unfortunately most common. As I teach my fellows the percent stenosis is the wrong way to think about lesions, rather we should say whether we believe a lesion to be flow limiting or not. Flow limitation is dependent on the stenosis but also on the reference vessel size, the lesion length, the size of the territory supplied by the vessel and the presence or absence of collaterals. The issue of interpretation is vital to the individual patient since it determines what treatment is recommended, You don't want a cardiologist to put in a stent or offer bypass surgery if your coronary artery lesion is not flow limiting. Recent studies have revealed what we knew all along namely that when coronary artery disease is moderate it is not possible to accurately know by visual assessment whether the lesion(s) are flow limiting or not. We need better methods not based on anatomy but rather on physiology. I have previously written about the RIPCORD trial but recently a large French registry has published its results which support the idea that the angiogram is difficult to interpret and that use of a pressure wire to measure fractional flow reserve (FFR) alters the cardiologists decision making. The R3F study looked at 1000 people having a diagnostic angiogram. The vessels were assessed and significant lesions documented. The patients symptoms and the results of any non-invasive investigations were considered and a recommendation made as to whether the patient should have medical therapy, angioplasty or bypass surgery. After this the cardiologists performed a pressure wire measurement (FFR) of any stenosis. The results were then used to determine whether the stenosis was flow limiting and with this information in hand the treatment recommendation adjusted. So for example if a patient had a 40% stenosis on the angiogram with medical therapy recommended initially but then the pressure wire was significant (e.g. FFR 0.74) the recommended treatment would be to offer an angioplasty. Using the pressure wire data the overall number of people recommended for medical therapy, angioplasty or bypass did not change but the decision for an individual patient changed 43% of the time. Overall the decision changed in 33% of patients initially recommended to have medical therapy and 50% of patients recommended to have angioplasty or bypass surgery. These results are very important for individual patients since the treatment recommendation means the difference between just taking tablets versus having a procedure or an operation. We don't know yet whether a pressure wire guided approach makes a difference to clinical endpoints such as survival, mortality, rates of heart attacks and a large trial is needed to answer this question. For the moment when a moderate stenosis is diagnosed the patient should be asking their cardiologist what is the FFR?  Dogs are out of control. Between 2009 and 2011 there was a 13% increase in the number of admissions to hospital due to dog attacks. A serious problem, dogs and their owners are out of control. Action must be taken!
But what does this 13% actually mean? What is it 13% of? In 2009/10 there were 5,837 admissions to hospital due to dog attacks. In 2011/12 the number was 6,580. That's an increase in 13 % or 743 cases. Is this a big problem for the NHS or society in general? In order to work that out we need to know the number of hospital admissions. In 2009/10 there were 6,430,372. This means that dog attacks represent 1 in 10,000 admissions. So a 13% increase is an increase from 0.0118% to 0.103%. This means that we are dealing with very small numbers which are unlikely to be of much clinical significance. The same caution needs to be applied to other hospital statistics. Take for example the current debate about weekend working in the NHS. This has been fuelled by studies indicating that the risk of dying is greater if you are admitted to hospital at the weekend compared to a weekday. This is shown in a recent study which reported that the 30 day mortality was 16% greater if you are admitted at the weekend. But what does this mean? Is it for every 100 deaths during the week there are 116 at the weekend. We need to analyse the data further. 14.2 million people were admitted to hospital in 2009/10 and 187,337 died. This means that 1.3% of people admitted died. The rate of death if you were admitted at the weekend was 16% higher, in other words about 0.21%. This means that the chance of dying within 30 days of admission is 0.21% higher if you are admitted at the weekend compared to a weekday. Alternatively there is a 98% chance of survival if admitted on a weekday compared to a 97.68% chance if admitted at the weekend. Is this clinically significant? I would welcome your comments.  In 1964 Nico Jacobellis, the manager of the Heights Art Theatre in Cleveland, Ohio was convicted of obscenity for showing a French film called Les Amants. The state deemed the film obscene but Jacobellis appealed to the US Supreme Court. They ruled the film was not obscene but the judges could not agree why. Famously, Justice Potter Stewart wrote of obscenity, "I shall not today attempt further to define the material I understand to be embraced within that shorthand description….but I know it when I see it." In medicine you often “know it when you see it." This might also be referred to as “clinical acumen” or the “end of the bed test” and one area this is often used is in the assessment of frailty.
The frail elderly are by definition weak and delicate and its consideration of frailty and the impact on decision making is growing in importance in cardiology due to the aging population. Take the treatment of non ST elevation myocardial infarction (NSTEMI). It is highly researched with clearly defined evidence based treatment protocols. Diagnosis is made with clinical history, ECG and troponin. There follows the prescription of potent anti-platelet/anti-thrombotic and then often angiography and for some percutaneous coronary intervention (PCI), Whilst we might debate the benefits of PCI in patients with stable angina, beyond reduction in symptoms, this is not in question in heart attack patients. Just in case you’re wondering about the evidence the Cochrane Review of the 4 major trials comparing a conservative to PCI strategy in NSTEMI showed no effect on overall mortality but reduced rates of refractory angina and re-hospitalization in the shorter term and myocardial infarction (MI) in the longer term. The PCI strategy was associated with a doubling in the risk of procedure-related MI and increased risk of bleeding. What all this is really saying is that if you stent a coronary narrowing now you are less likely to have to do it later. But there is a catch with these clinical trials. How many included patients who were 86 years old, walking with a frame, weak because of low muscle mass and on more than a dozen medications for all sorts of other medical problems, How many of these patients were frail elderly people. Of course very few since this type of patient isn’t able to comply with rigors of a clinical trial and are not attractive to the research team. Most trial patients are younger, with less co-morbidity, able to attend for follow up visits and able to consent they are good trial patients. Our problem is that the frailer patients occupy an increasing part of our workload. These patients have cardiac problems but this is in addition to problems are about being able to walk to the toilet, being able to bathe, the loss of independence, fear of what the future may hold, worry about their elderly spouse or whose going to look after the cat. There has been a trend in over the last 5 years for such elderly patients to be managed more by specialists rather than generalists or geriatricians. This makes it reasonable to ask whether we (cardiologists as a group) are well equipped to care for such patients with complex medical needs beyond having a blinkered view and focusing only on the heart. We may also fall into the trap of regarding these patients with therapeutic nihilism and therefore to deny the application of invasive therapies on the basis that the patient is too frail to withstand the procedure. Yet by definition such patients have the highest risk of death of all we treat and therefore may potentially have the greatest benefit. Weighing up the risks and benefits is difficult since measurement of both is uncertain. In the absence of clinical trials we look to registries and observational studies to try and fill in the evidence gaps. But caution is required since these are non-randomized studies and the risk of bias, even after the usual multivariate regression of all potential confounders has been applied, is strong. A paper just published in Heart illustrates this. The authors looked NSTEMI management and frailty. The study from Italy followed 698 patients with a mean age of 83 years. A quarter had ST elevation and the rest non-ST elevation MI and each patient was scored using the Silver Code (SC) frailty score. There are over 25 different scores of frailty all of them have their pros and cons. The SC is heavily weighted by age and a diagnosis of cancer and a SC score of ≥11 is used to define a person as frail. In the study 50% of patients were treated with PCI the rest with medical therapy. There are no surprises that if you had a STEMI and were admitted to a hospital that could do 24/7 PCI on site you were more likely to get a PCI. We all know that if the patient is delivered direct to the catheter laboratory the threshold for performing angiography and hence PCI is very low compared to a patient who is paid free and seen 48h after admission in a peripheral hospital without PCI facilities on site. The PCI patients were younger, male, had less heart failure, less anaemia and we less likely to have renal failure. In other words they had less co-morbidity. For every 1 point the SC score increased the chance of the patient having PCI decreased by 11%. The authors followed the outcome of the patients over the next year and used mortality as their end point. This is good because it is straightforward, simple to measure and meaningful. They found that PCI did not reduce the risk of death in people with a low SC score (0–3) but the benefit increased as the score increased such that people with a SC score of ≥11 had a 74% reduction in risk if they had a PCI. The conclusion from this study was that cardiologists are not offering treatment to the frail elderly who are in fact the very patients who benefit most from the procedure. Of course there is another explanation and that is the frail patients with an SC score of ≥11 were a heterogeneous group with some more frail than other. Those who got PCI were different even after adjustment for factors such as renal function, heart failure and age. As Justice Potter said “I know it when I see it.” The decision to refer the patient for PCI is made not just on administrative factors such as age, creatinine and number of medications but on a holistic assessment of the patient balancing the risk and benefit of the procedure with outcome for the patient. What we really need is a randomised study with mortality as its end point to address the question of PCI in very elderly presenting with MI until then clinical acumen will have to do.  "Everyone over 40 years old should take a statin - men and women." Those are not my words but those of Professor Sir Magdi Yacoub who is one of the world's most eminent heart surgeons. Interviewed on the Today program this morning he, with typical surgical aplomb, stated his opinion. When asked if every man over 50 should be on a statin he replied. "Definitely, I would say every man over 40" and what about for women Justin Webb asked, "Yes women too." So that's clear according to the Professor everyone over 40 should have a statin and not to do this he said was lunacy.
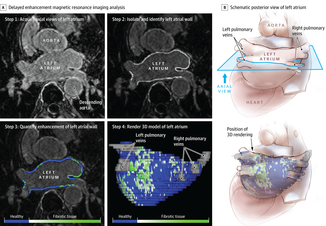
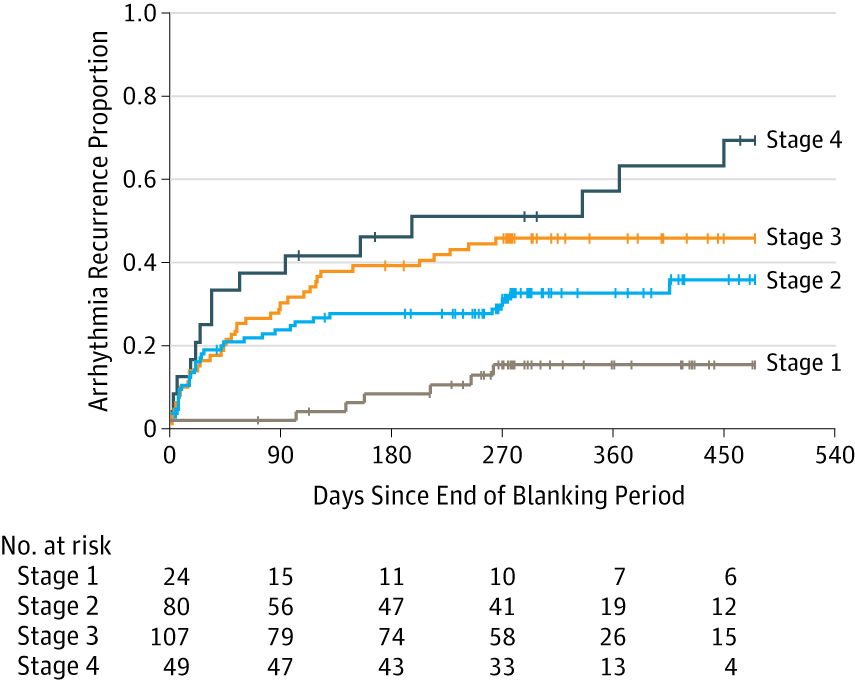
We are in a statin war, being played out on the media battlefield. Each side lobbing studies and statistics at each other across the 7 million people who take these drugs every day and the millions more who some think ought to. People are confused by these disagreements between the doctors as the two sides rage against each other. Into this toxic mix there is distrust of pharmaceutical companies, conflicts of interest and self-promotion amongst researchers and the wider social issues about the medicalization of the population. Today was an minor assault by the Statinistas. Deploying a "big gun" in the form of Sir Magdi to state the case for statins. A generous dose of eminence-based medicine was administered aurally. Yacoub said that if the cholesterol is low then this would result in not only reduced rates of heart attack and strokes but also reduction in dementia and cancer. He said "If the cholesterol is extremely low then people look very young at an old age and lead a long and happy life, so not to take statins is a disaster." Linking observations made in people with a very rare genetic cause of extremely low cholesterol (PCSK-9 deficiency) to the effects you would expect from taking statins seems somewhat absurd and stretches the evidence on statins into new orbits. Even the most ardent trialists would be likely to agree that currently body of statin data does not support Yacoub's views. But rather than speculation about the a cure for cancer or dementia the most provocative statement he made was that everyone over 40 should be on a statin. This is a debate about risk versus benefit. A debate about populations versus individuals. There is the strongest evidence that statins reduce the risk of heart attack and stroke. That cannot be denied. The reduction in risk is about 30%. The benefit is not dependent on the baseline level of cholesterol. If your risk is high you get a lot of benefit, if your risk is low, you benefit, but not so much. A simple way to express this is the "Number Needed to Treat" or NNT. If the NNT is large then the treatment is not very effective in that group of patients and may approach the Number Needed to Harm. In other words if you treat a large group of people at low risk then you may help a few and harm a few. The problem here is deciding at what level of risk to offer treatment. For statins in primary prevention the NNT is 60 for heart attack and 260 for stroke. In people with established heart disease the NNT is 39 to prevent a heart attack, 125 to prevent a stroke and 83 to save a life. To the individual patient these seem like high numbers but when you consider that millions of people are on statins then they rapidly multiply making the reduction in heart attacks, stroke and death look impressive. But we also need to keep in mind that giving statins for prevention where the risk is low is totally different from using them in high risk people. If we expose a large number of people to a small risk from the statin treatment then this is likely to yield more problems than if we were to expose a small number to a much bigger risk. The classical argument about treating populations was put forward by Geoffrey Rose in his book and articles on the Strategy of Preventative Medicine. Rose argues that a mass approach is the only ultimate answer to the problems of a mass disease. But, however much it offers to the population as a whole, it benefits each participating individual very little. Take the example of diphtheria immunisation. 600 children need to be immunised in order that one life would be saved. In other words 599 wasted immunisations were given. The same case may be made over seat belts where the number of times a seat belt needs to be worn to prevent one fatality is about 25,000. This is the prevention paradox. The effectiveness you have to accept in mass medicine where the measure applied to many will actually benefit few. A measure that brings large benefits to the community offers little to each participating individual. As Rose says: "We should not expect too much from health education as people won't be motivated to take the advice because there is little in it for them especially in the short term." So should you take a statin if your over 40 years old. Well it depends on your risk of cardiovascular disease compared to the average 40 year old. If you are at low risk because you don't smoke, your cholesterol and blood pressure are normal and you are otherwise healthy your benefit is very small. You may wish to take a statin and in that case either your doctor will prescribe it or you can buy 10mg simvastatin over the counter - it's your choice. If you are at increased risk compared to the average 40 year old because of raised blood pressure or elevated cholesterol then your benefit is higher and you are likely to be advised by your doctor to take a statin. Again it's your choice but the choice needs to be made after a proper discussion and the advice individualised and explained by someone with expertise in guiding the patient thought the arguments. Simply telling everyone over 40 to take statins is in the words of the Professor lunacy. 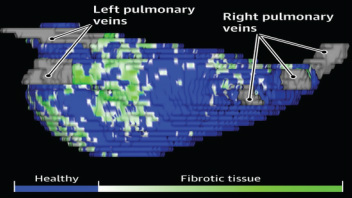 The success of ablation for atrial fibrillation (AF) is variable. It depends on the patient, it depends on the doctor. Traditional thinking was that people with a structurally normal heart on echo who had paroxysmal AF would do well with ablation. Those people with dilated left atrium and long standing persistent AF would not do so well. But how good are we really at selecting who will benefit from ablation? Pulmonary vein isolation (PVI) also known as AF ablation is the commonest catheter based procedure for the treatment of AF. The aim is to electrically isolate the pulmonary veins from the atrium because it is believed that ectopic beats arising in these veins are responsible for triggering episodes of AF. Despite the enthusiasm of some cardiologists for this procedure and the very large number of ablation procedures carried out daily around the world the long term results of randomised clinical trials are mixed to say the least with many patients relapsing back into AF within a year or requiring multiple procedures. Despite the best efforts of cardiologists the current clinical parameters we assess fail to define properly which patients will have successful maintenance of sinus rhythm after an AF ablation. Recent work performed at the University of Utah however is allowing us to think about the selection question differently. For a long time we have known that fibrosis in the atrium is important. The difficulty is how to measure fibrosis in people non-invasively. The Utah group have developed a method for assessing the amount of fibrosis in the left atrium using MR scanning. Using this information they are then able to show that the amount of fibrosis predicts which patients will respond well to ablation and remain free of AF and which patients will have a recurrence. The DECAAF study recently published in JAMA looked at 329 patients about two thirds of whom had paroxysmal AF and the rest persistent. They performed a special sequenced MR scan on all the patients. In 83% it was possible to obtained a scan of good enough quality to interpret. These patients then had an AF ablation were followed up for at least a year. At the end of the study about a quarter of patients were still on Class I or III (i.e. potent) anti-arhhythmic drugs indicating that ablation even if successful is does not mean no need for medication. Also about 5% of patients had a serious complication from the procedure. The MRI technique measured the amount of left atrial fibrosis and this was strongly associated with AF recurrence after removal of confounding variables such as age, hypertension history etc. When the patients were looked at 325 days after the ablation those with stage 1 (<10% fibrosis) had an AF recurrence rate of 15.3%, those with stage 2 (10-20% fibrosis) had a recurrence rate of 32.6%. By stage 3 (20-30% fibrosis) 45.9% were back in AF and stage 4 (>30% fibrosis) 51.1% were in AF. By 475 day the recurrence rate for stage 1 was 15.3% still but the stage 4 patients had increased to 69.4%. The AF phenotype of the patients - paroxysmal versus persistent, young versus old, short versus long history of AF does not predict fibrosis and so a young patient with paroxysmal AF may have extensive fibrosis and therefore a very high risk of arrhythmia recurrence whereas another patient, older and with persistent AF may have little fibrosis and therefore have a very good chance of long term success with AF ablation. The only clinical parameter associated with fibrosis was hypertension. These results suggest that imaging of patients with AF before recommending interventions might improve the management. Allowing us to avoid procedure that are unlikely to benefit patients and to offer them to those with much to gain. I predict that we will see a rise in imaging and tissue characterisation of AF patients over the next few years.
How good are cardiologists at assessing the significance of a coronary narrowing on an angiogram. If your cardiologist tells you that your artery is 95% narrowed is that really true? A 3mm vessel narrowed by 95% means the lumen size is only 0.15mm wide. That's very small - smaller in fact than a standard angioplasty guide-wire (0.36mm) and so the wire should occlude the artery when it crosses the lesion - this rarely happens. Precise assessments of severity of coronary stenosis by angiography are unreliable. But how unreliable? Patients and cardiologists are fixated on the degree of coronary stenosis. Tell a patient his artery is 50% narrow he is worried, tell him it's 90% narrowed his is beside himself - it could block off at any time he thinks. Is a patient with a 60% stenosis in less trouble than someone with an 80% one? Rather than becoming fixated about the percentage stenosis of an artery I prefer to grade lesions as significant or non-significant. Significant lesions cause limitation of blood flow during exercise or stress, non-significant ones don't. Patients with significant lesions may have improved quality of life/symptoms improved by local lesion treatment with a stent or coronary bypass. Patients with non-significant lesions are better off with medical therapy and should avoid stents or bypass as they are unlikely to be beneficial. The discussions of significance require cardiologists to transform anatomical data derived from an angiogram into functional data which is dependent on length of lesion, severity of stenosis, presence of collaterals etc. When lesions are very severe or very mild cardiologists will agree when asked to grade the severity. When arteries are moderately diseased the agreement turns to disagreement. What we need is a functional assessment of lesion significance. This can be provided by pre-angiography investigation with tests such as nuclear perfusion imaging and stress echocardiography giving information about regional ischaemia. But NICE says we should move to angiography when the risk of underlying coronary artery disease is more than 60% and so often patients find themselves having an invasive angiogram as the first line investigation in the absence of any information about coronary ischaemia. 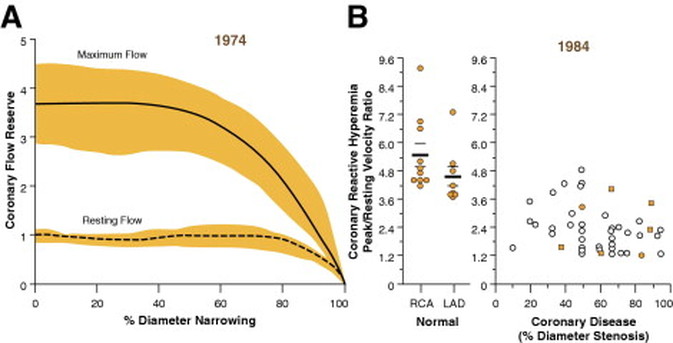 This week sees the publication of the RIPCORD trial which is a UK based study which looked at the role of pressure wire assessment to guide therapy of coronary artery disease. The group took 200 patients with angina and performed coronary angiography. A cardiologist formulated a management plan of either medical therapy, angioplasty, bypass surgery or unable to make a decision with further information required. At that point a second cardiologist came in an performed an FFR measurement with a pressure wire. After this the results were shared with the first cardiologist to see whether this altered the management plan for the patient.
The good news is that 74% of the time the management plan didn't change after the FFR measurement. In 72 patients medical treatment was recommended. In 9 patients revascularization was recommended after the FFR test (6 PCI, 3 CABG). In contrast, 25 patients who had been recommended for revascularization after angiogram (24 PCI, 1 CABG) were switched to medical therapy after the FFR data became available. In the total group of 200 cases after an angiogram 90 were led to the recommendation of PCI to ≥1 vessel, but in 24 (26.7%) there was no physiologically significant stenosis detected by FFR. So a quarter of patients recommended for an angioplasty did not have evidence of flow limiting disease and therefore the procedure would have been potentially worthless. So what does all this mean. First cardiologists can predict lesion significance from an angiogram in about 75% of cases. In fact that is not bad an it would be very interesting to see in this study if some cardiologists were better than others at making this prediction. My guess is there would be. Second it means that we are recommending some patients to have medical therapy when they would be benefit from revascularisation and we are subjecting some patients to invasive or surgical treatments without any reliable evidence that their coronary arteries are significantly narrowed. An approach to use the FFR measurement more widely gets the right treatment for the right patient. But this comes at a cost of about £450 extra per case because the pressure wire adds an expense to the angiogram. Second the complication rate from an FFR procedure is higher than that of diagnostic angiography and some patients with non-flow limiting lesions may sustain a complication such as coronary dissection which requires emergency surgery or stenting. Overall we should move to a more accurate way of diagnosing coronary artery disease and being able to assess lesions in detail at the time of angiography is likely to gain momentum. Cardiologists need to stop kidding themselves and their patients that they can assess the significance of a coronary stenosis accurately every time.  In the last 10 years the number of people with type 2 diabetes in England has increased by a million. by 2013 in England 1 in 20 people were diabetic. That is over five and a half million people or put another way the same as all the people who work in the public sector in the UK or the population of Manchester and the West Midlands combined.
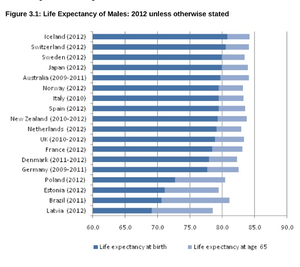
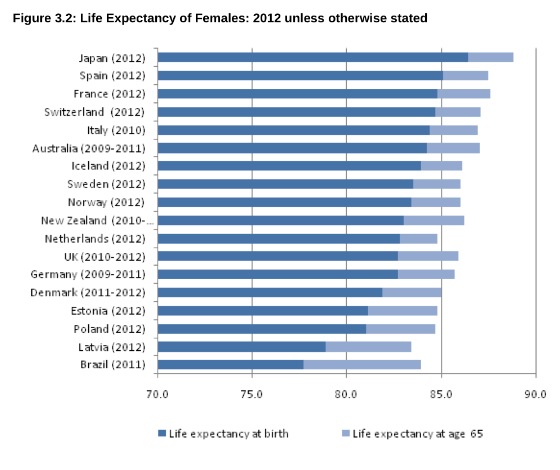
Diabetes is a serious condition associated with an increased risk of heart and vascular disease, blindness and kidney failure. To put it in perspective your risk of having a heart attack if you are diabetic is the same as the risk of a person who has already had one heart attack having another one. We take diabetes seriously and spend a lot of time trying to prevent complications from condition. We also try to prevent diabetes by telling people about the lifestyle changes which will reduce their risk. In England every adult aged 40 to 74 is offered a NHS Health check designed to detect obesity, diabetes, high blood pressure and raised cholesterol. Doctors are told to calculate a patients cardiovascular risk and decide whether to prescribe statins. Originally the threshold of risk for statin prescription was 30%, then a few years later, when branded statins came off patent, it was lowered to 20% and soon, if new draft NICE guidelines go through, it will be lowered to 10%. As the prescription of statins has moved from people with established medical problems to those simply at risk concerns have been raised about the threat of medicalising the population. With this there has been growing worry about the unintended effects of statins. What has emerged is that statins definitely cause muscle problems and abnormalities of liver function tests but more worryingly there is growing evidence that statins cause diabetes. Randomized controlled trials prove that statins reduce risk of cardiovascular disease by 30%. This is an impressive number but remember the absolute benefit for an individual patient is absolutely determined by their actual risk of heart disease. If this number is low then the absolute benefit will also be low, 30% of a very small number is still a very small number. So in lower risk people the clinical benefit may be balanced or even outweighed by potential harm from unintended effects. A recent meta-analysis suggested that statins are associated with a 9% increased relative risk of diabetes and a systematic review reported an odds ratio of 1.31 for the development of diabetes. Another analysis of 5 statin trials with 32,752 participants without diabetes at baseline showed that 2749 developed diabetes (2.0 extra cases/1000 patient-years) with an odds ratio of 1.12 for new-onset diabetes. In women where the beneficial effects of statins are less clear, the Women’s Health Initiative study reported evidence of increased risk of diabetes with a number needed to harm of 44 patients for an additional case of diabetes over three years of treatment. We think the diabetes epidemic is related to the rising tide of obesity and slothfulness but could it be that the increase is being driven by the prescription of statins which have reached epidemic proportions over the last 10 years. In 2013 doctors wrote 63 million prescriptions for over 2.13 billion statins tablets in England. If being on a statin increases the risk of diabetes and we use the conservative estimate of 2 cases per 1000 patient year then because the number of people statins are prescribed to is so large (5.84 million people taking statins) we could expect at least 12,000 extra cases of diabetes to occur as a direct result of the statin treatment. A more pessimistic scenario based on the Women's Health Initiative number needed to harm of 44 would predict an extra 133,000 cases of diabetes as a direct result of statin treatment. The number of people with diabetes is rising by about 140,000 per year. Now association does not prove causation but the trend rise in diabetes and statin prescribing is worrying and should make doctors thick twice when recommending statin treatment to people at lower cardiovascular risk where the potential for harm from the treatment might outweigh the potential for benefit. Diabetes is now very common so doctors will never be surprised when new cases occur especially in people who are taking statins, after all these are the people at risk of cardiovascular disease in whom diabetes is likely to be prevalent anyway. Individual doctors will miss the association between diabetes and statins because the background level of the diabetes is very high. It is much easier to identify unwanted effects of a drug if it causes a rare or unusual effect because these events stand out. So we need to think carefully about the balance of risk and benefit when we prescribe statins, after all we need to ensure that overall the patient is likely to benefit from the treatment rather than be harmed by it especially if their underling cardiovascular risk is low.  Friday 25th April 2014- The Times, front page news, above the crease. The story must be important. It is they have discovered the "Secret of longer life". Here is the skill of the journalist. Take a study just published. Read it and Identify one fact from all the results which makes the hook for the story. In this case Japanese women have the highest life expectancy. Then find a plausible association. What do we know about Japan? Ah well Sushi? - that's raw fish and Green Tea? Well that must be the cause of the long survival and there it is you have your story and your headline and your front page. So what lies behind this news and is there any credibility in the conclusion. The Office for National Statistics published an international Compendium of Data on population statistics today. Much of the report will fuel the current debate around UK immigration as there is a substantial amount of data on population migration and enough material in the report to satisfy the needs of the pro as well as the anti-European debate and to prove either groups case! The life expectancy data comes later and leads to the headline. Well I'm sorry to have to disappoint but I am afraid that the secret of longer life isn't about raw fish or green tea. Sadly the journalists haven't been entirely transparent with the facts. It is true that Japanese females do have the highest life expectancy at birth (86.4 years) but the country with the highest male life expectancy at birth at 80.8 years was Iceland.
Now it is true they eat a lot of fish in Iceland. In fact a recent FAO report indicates that the annual fish consumption in Iceland is 80.5kg/year compared to just 55.2 in Japan. So you could ask if fish in the diet was so important why didn't the Icelandic women top the Japanese. Well perhaps it's the type of fish, or the way it's cooked or not cooked. More likely perhaps this is simply an association which tells you nothing about causation. It could be the play of chance or any number of other factors which confound the association between the diet and life expectancy. its almost as bizarre as thinking that the amount of chocolate you eat determines the chance of winning a Nobel prize. 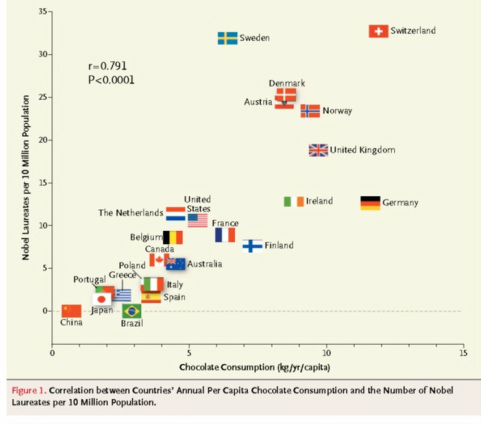
 The old saying goes you should breakfast like a King, lunch like a Prince and dine like a pauper. Breakfast may be the most important meal of the day but now it turns out that it's effects reach far beyond the breakfast table.
What you eat for breakfast influences not only how full you feel at the time but how much food you eat for lunch and dinner. So what's the best breakfast? A poached egg, a bowel of cereal and a slice of toast or something more continental - a croissant with butter and jam perhaps? Researchers at the University of Surrey have been looking at whether what you eat at breakfast alters how hungry you feel later in the day. They randomly assigned three groups of students to different breakfasts all containing 330 kilocalories. The breakfasts were either two poached eggs on a slice of white toast or a bowl of cornflakes with semi-skimmed milk, a slice of white toast or a croissant with butter and jam and orange juice. For lunch the students were offered a buffet of cheese sandwiches, plain crisps and water. For dinner they were offered a buffet of pasta and a tomato sauce and cheese and water. The amount of lunch and dinner they took from the buffet was recorded as were scores of hunger and fullness during the day. Their results showed that the egg breakfast made people feel significantly fuller for longer and reduced the amount of lunch and dinner taken from the buffet. The proportion of fat and protein in the egg breakfast was higher and the carbohydrate content lower than the other breakfasts. It is known that high-protein foods make you feel fuller than high fat or carbohydrate ones and show the importance of food choice at breakfast. But hold on I hear you say can a cardiologist really be recommending that people eat eggs. In the 1960's the Egg Marketing Board ran a highly successful campaign called "Go to work on an Egg" but with the demonization of saturated fat in the 1970's and 80's, eggs with their high cholesterol content were rejected in favour of high carbohydrate breakfast cereals. Well it turns out that your more likely to raise your cholesterol by eating butter on your toast than from the cholesterol in an egg. In a large meta-analysis published in the BMJ looking at 17 reports on data from 4 million people there was no evidence of an association between egg consumption and risk of coronary heart disease or stroke and now even the British Heart Foundation is now promoting the consumption of eggs. So this means you can go to work on an egg if you want to and it might well help you lose weight by reducing the size of your lunch and dinner. |

Dr Richard BogleThe opinions expressed in this blog are strictly those of the author and should not be construed as the opinion or policy of my employers nor recommendations for your care or anyone else's. Always seek professional guidance instead. Archives
August 2023
Categories
All

|

 RSS Feed
RSS Feed