 In 1964 Nico Jacobellis, the manager of the Heights Art Theatre in Cleveland, Ohio was convicted of obscenity for showing a French film called Les Amants. The state deemed the film obscene but Jacobellis appealed to the US Supreme Court. They ruled the film was not obscene but the judges could not agree why. Famously, Justice Potter Stewart wrote of obscenity, "I shall not today attempt further to define the material I understand to be embraced within that shorthand description….but I know it when I see it." In medicine you often “know it when you see it." This might also be referred to as “clinical acumen” or the “end of the bed test” and one area this is often used is in the assessment of frailty.
The frail elderly are by definition weak and delicate and its consideration of frailty and the impact on decision making is growing in importance in cardiology due to the aging population. Take the treatment of non ST elevation myocardial infarction (NSTEMI). It is highly researched with clearly defined evidence based treatment protocols. Diagnosis is made with clinical history, ECG and troponin. There follows the prescription of potent anti-platelet/anti-thrombotic and then often angiography and for some percutaneous coronary intervention (PCI), Whilst we might debate the benefits of PCI in patients with stable angina, beyond reduction in symptoms, this is not in question in heart attack patients. Just in case you’re wondering about the evidence the Cochrane Review of the 4 major trials comparing a conservative to PCI strategy in NSTEMI showed no effect on overall mortality but reduced rates of refractory angina and re-hospitalization in the shorter term and myocardial infarction (MI) in the longer term. The PCI strategy was associated with a doubling in the risk of procedure-related MI and increased risk of bleeding. What all this is really saying is that if you stent a coronary narrowing now you are less likely to have to do it later. But there is a catch with these clinical trials. How many included patients who were 86 years old, walking with a frame, weak because of low muscle mass and on more than a dozen medications for all sorts of other medical problems, How many of these patients were frail elderly people. Of course very few since this type of patient isn’t able to comply with rigors of a clinical trial and are not attractive to the research team. Most trial patients are younger, with less co-morbidity, able to attend for follow up visits and able to consent they are good trial patients. Our problem is that the frailer patients occupy an increasing part of our workload. These patients have cardiac problems but this is in addition to problems are about being able to walk to the toilet, being able to bathe, the loss of independence, fear of what the future may hold, worry about their elderly spouse or whose going to look after the cat. There has been a trend in over the last 5 years for such elderly patients to be managed more by specialists rather than generalists or geriatricians. This makes it reasonable to ask whether we (cardiologists as a group) are well equipped to care for such patients with complex medical needs beyond having a blinkered view and focusing only on the heart. We may also fall into the trap of regarding these patients with therapeutic nihilism and therefore to deny the application of invasive therapies on the basis that the patient is too frail to withstand the procedure. Yet by definition such patients have the highest risk of death of all we treat and therefore may potentially have the greatest benefit. Weighing up the risks and benefits is difficult since measurement of both is uncertain. In the absence of clinical trials we look to registries and observational studies to try and fill in the evidence gaps. But caution is required since these are non-randomized studies and the risk of bias, even after the usual multivariate regression of all potential confounders has been applied, is strong. A paper just published in Heart illustrates this. The authors looked NSTEMI management and frailty. The study from Italy followed 698 patients with a mean age of 83 years. A quarter had ST elevation and the rest non-ST elevation MI and each patient was scored using the Silver Code (SC) frailty score. There are over 25 different scores of frailty all of them have their pros and cons. The SC is heavily weighted by age and a diagnosis of cancer and a SC score of ≥11 is used to define a person as frail. In the study 50% of patients were treated with PCI the rest with medical therapy. There are no surprises that if you had a STEMI and were admitted to a hospital that could do 24/7 PCI on site you were more likely to get a PCI. We all know that if the patient is delivered direct to the catheter laboratory the threshold for performing angiography and hence PCI is very low compared to a patient who is paid free and seen 48h after admission in a peripheral hospital without PCI facilities on site. The PCI patients were younger, male, had less heart failure, less anaemia and we less likely to have renal failure. In other words they had less co-morbidity. For every 1 point the SC score increased the chance of the patient having PCI decreased by 11%. The authors followed the outcome of the patients over the next year and used mortality as their end point. This is good because it is straightforward, simple to measure and meaningful. They found that PCI did not reduce the risk of death in people with a low SC score (0–3) but the benefit increased as the score increased such that people with a SC score of ≥11 had a 74% reduction in risk if they had a PCI. The conclusion from this study was that cardiologists are not offering treatment to the frail elderly who are in fact the very patients who benefit most from the procedure. Of course there is another explanation and that is the frail patients with an SC score of ≥11 were a heterogeneous group with some more frail than other. Those who got PCI were different even after adjustment for factors such as renal function, heart failure and age. As Justice Potter said “I know it when I see it.” The decision to refer the patient for PCI is made not just on administrative factors such as age, creatinine and number of medications but on a holistic assessment of the patient balancing the risk and benefit of the procedure with outcome for the patient. What we really need is a randomised study with mortality as its end point to address the question of PCI in very elderly presenting with MI until then clinical acumen will have to do.
0 Comments
 "Everyone over 40 years old should take a statin - men and women." Those are not my words but those of Professor Sir Magdi Yacoub who is one of the world's most eminent heart surgeons. Interviewed on the Today program this morning he, with typical surgical aplomb, stated his opinion. When asked if every man over 50 should be on a statin he replied. "Definitely, I would say every man over 40" and what about for women Justin Webb asked, "Yes women too." So that's clear according to the Professor everyone over 40 should have a statin and not to do this he said was lunacy.
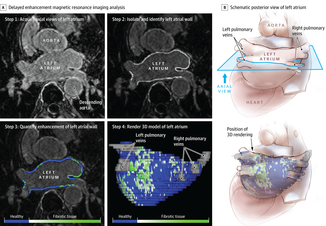
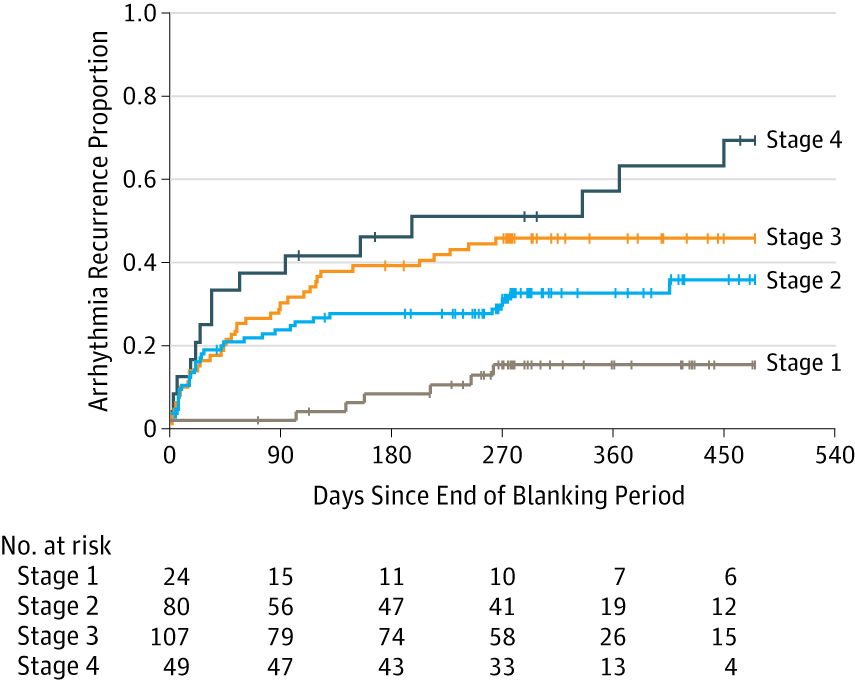
We are in a statin war, being played out on the media battlefield. Each side lobbing studies and statistics at each other across the 7 million people who take these drugs every day and the millions more who some think ought to. People are confused by these disagreements between the doctors as the two sides rage against each other. Into this toxic mix there is distrust of pharmaceutical companies, conflicts of interest and self-promotion amongst researchers and the wider social issues about the medicalization of the population. Today was an minor assault by the Statinistas. Deploying a "big gun" in the form of Sir Magdi to state the case for statins. A generous dose of eminence-based medicine was administered aurally. Yacoub said that if the cholesterol is low then this would result in not only reduced rates of heart attack and strokes but also reduction in dementia and cancer. He said "If the cholesterol is extremely low then people look very young at an old age and lead a long and happy life, so not to take statins is a disaster." Linking observations made in people with a very rare genetic cause of extremely low cholesterol (PCSK-9 deficiency) to the effects you would expect from taking statins seems somewhat absurd and stretches the evidence on statins into new orbits. Even the most ardent trialists would be likely to agree that currently body of statin data does not support Yacoub's views. But rather than speculation about the a cure for cancer or dementia the most provocative statement he made was that everyone over 40 should be on a statin. This is a debate about risk versus benefit. A debate about populations versus individuals. There is the strongest evidence that statins reduce the risk of heart attack and stroke. That cannot be denied. The reduction in risk is about 30%. The benefit is not dependent on the baseline level of cholesterol. If your risk is high you get a lot of benefit, if your risk is low, you benefit, but not so much. A simple way to express this is the "Number Needed to Treat" or NNT. If the NNT is large then the treatment is not very effective in that group of patients and may approach the Number Needed to Harm. In other words if you treat a large group of people at low risk then you may help a few and harm a few. The problem here is deciding at what level of risk to offer treatment. For statins in primary prevention the NNT is 60 for heart attack and 260 for stroke. In people with established heart disease the NNT is 39 to prevent a heart attack, 125 to prevent a stroke and 83 to save a life. To the individual patient these seem like high numbers but when you consider that millions of people are on statins then they rapidly multiply making the reduction in heart attacks, stroke and death look impressive. But we also need to keep in mind that giving statins for prevention where the risk is low is totally different from using them in high risk people. If we expose a large number of people to a small risk from the statin treatment then this is likely to yield more problems than if we were to expose a small number to a much bigger risk. The classical argument about treating populations was put forward by Geoffrey Rose in his book and articles on the Strategy of Preventative Medicine. Rose argues that a mass approach is the only ultimate answer to the problems of a mass disease. But, however much it offers to the population as a whole, it benefits each participating individual very little. Take the example of diphtheria immunisation. 600 children need to be immunised in order that one life would be saved. In other words 599 wasted immunisations were given. The same case may be made over seat belts where the number of times a seat belt needs to be worn to prevent one fatality is about 25,000. This is the prevention paradox. The effectiveness you have to accept in mass medicine where the measure applied to many will actually benefit few. A measure that brings large benefits to the community offers little to each participating individual. As Rose says: "We should not expect too much from health education as people won't be motivated to take the advice because there is little in it for them especially in the short term." So should you take a statin if your over 40 years old. Well it depends on your risk of cardiovascular disease compared to the average 40 year old. If you are at low risk because you don't smoke, your cholesterol and blood pressure are normal and you are otherwise healthy your benefit is very small. You may wish to take a statin and in that case either your doctor will prescribe it or you can buy 10mg simvastatin over the counter - it's your choice. If you are at increased risk compared to the average 40 year old because of raised blood pressure or elevated cholesterol then your benefit is higher and you are likely to be advised by your doctor to take a statin. Again it's your choice but the choice needs to be made after a proper discussion and the advice individualised and explained by someone with expertise in guiding the patient thought the arguments. Simply telling everyone over 40 to take statins is in the words of the Professor lunacy. 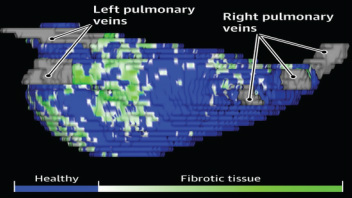 The success of ablation for atrial fibrillation (AF) is variable. It depends on the patient, it depends on the doctor. Traditional thinking was that people with a structurally normal heart on echo who had paroxysmal AF would do well with ablation. Those people with dilated left atrium and long standing persistent AF would not do so well. But how good are we really at selecting who will benefit from ablation? Pulmonary vein isolation (PVI) also known as AF ablation is the commonest catheter based procedure for the treatment of AF. The aim is to electrically isolate the pulmonary veins from the atrium because it is believed that ectopic beats arising in these veins are responsible for triggering episodes of AF. Despite the enthusiasm of some cardiologists for this procedure and the very large number of ablation procedures carried out daily around the world the long term results of randomised clinical trials are mixed to say the least with many patients relapsing back into AF within a year or requiring multiple procedures. Despite the best efforts of cardiologists the current clinical parameters we assess fail to define properly which patients will have successful maintenance of sinus rhythm after an AF ablation. Recent work performed at the University of Utah however is allowing us to think about the selection question differently. For a long time we have known that fibrosis in the atrium is important. The difficulty is how to measure fibrosis in people non-invasively. The Utah group have developed a method for assessing the amount of fibrosis in the left atrium using MR scanning. Using this information they are then able to show that the amount of fibrosis predicts which patients will respond well to ablation and remain free of AF and which patients will have a recurrence. The DECAAF study recently published in JAMA looked at 329 patients about two thirds of whom had paroxysmal AF and the rest persistent. They performed a special sequenced MR scan on all the patients. In 83% it was possible to obtained a scan of good enough quality to interpret. These patients then had an AF ablation were followed up for at least a year. At the end of the study about a quarter of patients were still on Class I or III (i.e. potent) anti-arhhythmic drugs indicating that ablation even if successful is does not mean no need for medication. Also about 5% of patients had a serious complication from the procedure. The MRI technique measured the amount of left atrial fibrosis and this was strongly associated with AF recurrence after removal of confounding variables such as age, hypertension history etc. When the patients were looked at 325 days after the ablation those with stage 1 (<10% fibrosis) had an AF recurrence rate of 15.3%, those with stage 2 (10-20% fibrosis) had a recurrence rate of 32.6%. By stage 3 (20-30% fibrosis) 45.9% were back in AF and stage 4 (>30% fibrosis) 51.1% were in AF. By 475 day the recurrence rate for stage 1 was 15.3% still but the stage 4 patients had increased to 69.4%. The AF phenotype of the patients - paroxysmal versus persistent, young versus old, short versus long history of AF does not predict fibrosis and so a young patient with paroxysmal AF may have extensive fibrosis and therefore a very high risk of arrhythmia recurrence whereas another patient, older and with persistent AF may have little fibrosis and therefore have a very good chance of long term success with AF ablation. The only clinical parameter associated with fibrosis was hypertension. These results suggest that imaging of patients with AF before recommending interventions might improve the management. Allowing us to avoid procedure that are unlikely to benefit patients and to offer them to those with much to gain. I predict that we will see a rise in imaging and tissue characterisation of AF patients over the next few years.
How good are cardiologists at assessing the significance of a coronary narrowing on an angiogram. If your cardiologist tells you that your artery is 95% narrowed is that really true? A 3mm vessel narrowed by 95% means the lumen size is only 0.15mm wide. That's very small - smaller in fact than a standard angioplasty guide-wire (0.36mm) and so the wire should occlude the artery when it crosses the lesion - this rarely happens. Precise assessments of severity of coronary stenosis by angiography are unreliable. But how unreliable? Patients and cardiologists are fixated on the degree of coronary stenosis. Tell a patient his artery is 50% narrow he is worried, tell him it's 90% narrowed his is beside himself - it could block off at any time he thinks. Is a patient with a 60% stenosis in less trouble than someone with an 80% one? Rather than becoming fixated about the percentage stenosis of an artery I prefer to grade lesions as significant or non-significant. Significant lesions cause limitation of blood flow during exercise or stress, non-significant ones don't. Patients with significant lesions may have improved quality of life/symptoms improved by local lesion treatment with a stent or coronary bypass. Patients with non-significant lesions are better off with medical therapy and should avoid stents or bypass as they are unlikely to be beneficial. The discussions of significance require cardiologists to transform anatomical data derived from an angiogram into functional data which is dependent on length of lesion, severity of stenosis, presence of collaterals etc. When lesions are very severe or very mild cardiologists will agree when asked to grade the severity. When arteries are moderately diseased the agreement turns to disagreement. What we need is a functional assessment of lesion significance. This can be provided by pre-angiography investigation with tests such as nuclear perfusion imaging and stress echocardiography giving information about regional ischaemia. But NICE says we should move to angiography when the risk of underlying coronary artery disease is more than 60% and so often patients find themselves having an invasive angiogram as the first line investigation in the absence of any information about coronary ischaemia. 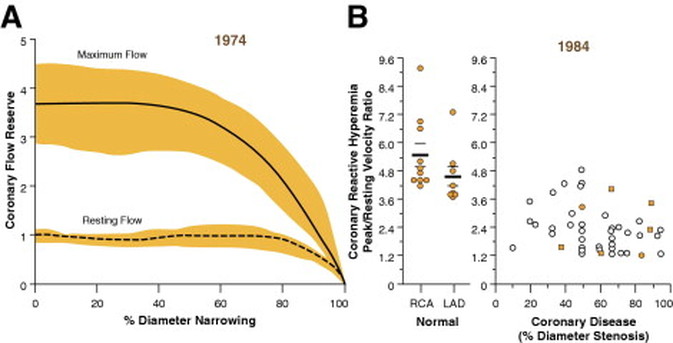 This week sees the publication of the RIPCORD trial which is a UK based study which looked at the role of pressure wire assessment to guide therapy of coronary artery disease. The group took 200 patients with angina and performed coronary angiography. A cardiologist formulated a management plan of either medical therapy, angioplasty, bypass surgery or unable to make a decision with further information required. At that point a second cardiologist came in an performed an FFR measurement with a pressure wire. After this the results were shared with the first cardiologist to see whether this altered the management plan for the patient.
The good news is that 74% of the time the management plan didn't change after the FFR measurement. In 72 patients medical treatment was recommended. In 9 patients revascularization was recommended after the FFR test (6 PCI, 3 CABG). In contrast, 25 patients who had been recommended for revascularization after angiogram (24 PCI, 1 CABG) were switched to medical therapy after the FFR data became available. In the total group of 200 cases after an angiogram 90 were led to the recommendation of PCI to ≥1 vessel, but in 24 (26.7%) there was no physiologically significant stenosis detected by FFR. So a quarter of patients recommended for an angioplasty did not have evidence of flow limiting disease and therefore the procedure would have been potentially worthless. So what does all this mean. First cardiologists can predict lesion significance from an angiogram in about 75% of cases. In fact that is not bad an it would be very interesting to see in this study if some cardiologists were better than others at making this prediction. My guess is there would be. Second it means that we are recommending some patients to have medical therapy when they would be benefit from revascularisation and we are subjecting some patients to invasive or surgical treatments without any reliable evidence that their coronary arteries are significantly narrowed. An approach to use the FFR measurement more widely gets the right treatment for the right patient. But this comes at a cost of about £450 extra per case because the pressure wire adds an expense to the angiogram. Second the complication rate from an FFR procedure is higher than that of diagnostic angiography and some patients with non-flow limiting lesions may sustain a complication such as coronary dissection which requires emergency surgery or stenting. Overall we should move to a more accurate way of diagnosing coronary artery disease and being able to assess lesions in detail at the time of angiography is likely to gain momentum. Cardiologists need to stop kidding themselves and their patients that they can assess the significance of a coronary stenosis accurately every time. |

Dr Richard BogleThe opinions expressed in this blog are strictly those of the author and should not be construed as the opinion or policy of my employers nor recommendations for your care or anyone else's. Always seek professional guidance instead. Archives
August 2023
Categories
All

|
 RSS Feed
RSS Feed